Lopes Freire GM, Espasa Suarez de Deza JE, Rodrigues da Silva IC Non-nutritive sucking habits and their effects on the occlusion in the deciduous dentition in children. Eur J Paediatr Dent. 2016; 17:301-306
Borrie FR, Bearn DR, Innes NP, Iheozor-Ejiofor Z. Interventions for the cessation of non-nutritive sucking habits in children. Cochrane Database Syst Rev. 2015; 3 https://doi.org/10.1002/14651858.CD008694.pub2
Nanda SK. Patterns of vertical growth in the face. Am J Orthod Dentofac Orthop. 1988; 93:103-116
Ellis E, McNamara JA Components of adult Class III open-bite malocclusion. Am J Orthod. 1984; 86:277-290
Harvold EP, Vargervik K, Chierici G. Primate experiments on oral sensation and dental malocclusions. Am J Orthod. 1973; 63:494-508
Linder-Aronson S. Effects of adenoidectomy on dentition and nasopharynx. Am J Orthod. 1974; 65:1-15
Linder-Aronson S, Woodside D, Lundströ A. Mandibular growth direction following adenoidectomy. Am J Orthod. 1986; 89:273-284
Bazargani F, Magnuson A, Ludwig B. Effects on nasal airflow and resistance using two different RME appliances: a randomized controlled trial. Eur J Orthod. 2018; 40:281-284 https://doi.org/10.1093/ejo/cjx081
El H, Palomo JM. Three-dimensional evaluation of upper airway following rapid maxillary expansion: a CBCT study. Angle Orthod. 2014; 84:265-273 https://doi.org/10.2319/012313-71.1
Cayley AS, Tindall AP, Sampson WJ, Butcher AR. Electropalatographic and cephalometric assessment of myofunctional therapy in open-bite subjects. Aust Orthod J. 2000; 16:23-33
Souza DRd, Semechini TA, Kröll LB, Berzin F. Oral myofunctional and electromyographic evaluation of the anterior suprahyoid muscles and tongue thrust in patients with Class II/1 malocclusion submitted to first premolar extraction. J Appl Oral Sci. 2007; 15:24-28
Wolford LM, Cottrell DA. Diagnosis of macroglossia and indications for reduction glossectomy. Am J Orthod Dentofacial Orthop. 1996; 110:170-177
Tanaka OM, Guariza-Filho O, Carlini JL Glossectomy as an adjunct to correct an open-bite malocclusion with shortened maxillary central incisor roots. Am J Orthod Dentofac Orthoped. 2013; 144:130-140 https://doi.org/10.1016/j.ajodo.2012.08.029
Farronato G, Salvadori S, Giannini L, Maspero C. Congenital macroglossia: surgical and orthodontic management. Progr Orthod. 2012; 13:92-98 https://doi.org/10.1016/j.pio.2011.06.003
Wang J, Goodger NM, Pogrel MA. The role of tongue reduction. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003; 95:269-273 https://doi.org/10.1067/moe.2003.1
Maisels DO, Knowles CC. Spontaneous regression of anterior open bite following treatment of macroglossia. Br J Plast Surg. 1979; 32:309-314 https://doi.org/10.1016/0007-1226(79)90087-0
Hikita R, Kobayashi Y, Tsuji M Long-term orthodontic and surgical treatment and stability of a patient with Beckwith–Wiedemann syndrome. Am J Orthod Dentofacial Orthop. 2014; 145:672-684 https://doi.org/10.1016/j.ajodo.2013.08.019
Lanigan DT, Hey JH, West RA. Aseptic necrosis following maxillary osteotomies: report of 36 cases. J Oral Maxillofac Surg. 1990; 48:142-156 https://doi.org/10.1016/S0278-2391(10)80202-2
Teemul TA, Perfettini J, Morris DO, Russell JL. Post-operative avascular necrosis of the maxilla: a rare complication following orthognathic surgery. J Surg Case Rep. 2017; 2017 https://doi.org/10.1093/jscr/rjw240
Liu ZJ, Shcherbatyy V, Perkins JA. Functional loads of the tongue and consequences of volume reduction. J Oral Maxillofac Surg. 2008; 66:1351-1361 https://doi.org/10.1016/j.joms.2007.11.005
Matsumoto K, Morita K-I, Jinno S, Omura K. Sensory changes after tongue reduction for macroglossia. Oral Surg Oral Med Oral Pathol Oral Radiol. 2014; 117:e1-e2 https://doi.org/10.1016/j.oooo.2012.02.037
Matsune K, Miyoshi K, Kosaki R Taste after reduction of the tongue in Beckwith–Wiedemann syndrome. Br J Oral Maxillofac Surg. 2006; 44:49-51 https://doi.org/10.1016/j.bjoms.2005.03.015
Maas SM, Kadouch DJ, Masselink A-CCM, Van Der Horst CMAM. Taste and speech following surgical tongue reduction in children with Beckwith–Wiedemann syndrome. J Cranio-Maxillofac Surg. 2016; 44:659-663 https://doi.org/10.1016/j.jcms.2016.02.010
Partial Glossectomy as an adjunct to Orthodontic Treatment of Anterior Open Bite Associated with Macroglossia: A Case Report Tarun K Mittal Kulraj Achal James T Taylor Jay D Kindelan Dental Update 2024 14:1, 707-709.
Orthodontic treatment of an anterior open bite is one of the most challenging malocclusions to treat, especially with respect to post-treatment stability. Complete diagnosis and targeted treatment is required for successful post treatment stability. In instances where macroglossia is the primary aetiology, partial glossectomy will greatly improve post treatment stability. The following case report describes a patient with severe anterior open bite and bimaxillary protrusion secondary to macroglossia. Treatment was successfully performed with partial glossectomy and straight wire orthodontics. Post-treatment relapse was minimal.
CPD/Clinical Relevance: This article describes a review of the aetiology of anterior open bite and documents one possible treatment option, when the main aetiology of the malocclusion is of soft tissue origin
Article
The successful treatment of anterior open bite is dependent on accurate diagnosis and correction of the aetiology. The development of anterior openbite (AOB) is multifactorial in nature and may be due to dental, skeletal or soft tissue causes or a combination of these factors.
Dental factors
Incomplete eruption of anterior teeth may result in an anterior open bite. Should the patient have potential for further eruptive change of the incisors, then monitoring would be prudent. Failure of eruption of incisors may result from the presence of supernumerary teeth impeding the eruption of incisors or as a result of bony replacement resorption (ankylosis) secondary to dento-alveolar trauma. Treatment may involve orthodontic or surgical repositioning, alveolar distraction in conjunction with orthodontics or extraction and replacement of the anteriortooth.1
Digit-sucking habits can cause anterior open bite development by impeding vertical eruption of incisors.2,3 Should the habit persist into adolescence, the posterior teeth may overerupt into contact – there will then be little chance of spontaneous improvement of the AOB, even with cessation of the habit.4
Skeletal factors
Vertical growth patterns can lead to the development of an anterior open bite, especially in patients with ‘long-face syndrome’.5,6 The vertical dimension of growth is thought to be secondary to constricted nasal airways and mouth breathing.7 It is postulated that adenoidectomy at an early stage may improve nasal airway space and encourage improvement in growth patterns.8,9 Some recent research has investigated the effect of rapid maxillary expansion on nasal airways in the early mixed dentition. Results of the most recent investigation10 comparing tooth-borne and tooth- and bone-borne expanders found that tooth- and bone-borne expanders resulted in a mean increase of 52.7 cm3/s in nasal airflow compared to tooth-borne expanders alone.10,11 Bone-borne expansion devices may, therefore, play a role in increasing nasal airflow in individuals thought to be affected by a constricted airway.
Intervention while a patient is still growing may potentially have an effect on the pattern and direction of growth, although long-term results are yet to be consistently reported. If growth has stopped, the only successful method of treatment will be surgical correction of the skeletal pattern with orthognathic surgery.12
Soft tissue factors
The soft tissues have a significant effect on the dentition and the development of the jaws.13,14,15 A commonly seen trait in patients with AOB is that of macroglossia with or without a tongue thrust. This can be adaptive or endogenous in nature, the former resolving following correction of the AOB, and the latter often causing significant relapse following the end of active treatment.16 While myofunctional appliances and tongue training may have a role in the correction of AOB during adolescence,17 treatment following completion of growth is complex.
The diagnosis of endogenous tongue thrust can often be made on clinical findings – symmetrical AOB in the absence of digit habit, presence of lisp, anterior positioning of tongue. Electromyography may be employed, but is of limited additional benefit.18 The diagnosis of macroglossia could be described as relative macroglossia when the mandible is retrognathic or deficient, giving the appearance of a large tongue although anatomical size is normal. Alternatively the clinical diagnosis of true macroglossia is mostly on the basis of clinical findings,19 particularly a broad or flat tongue, open bite, Class III malocclusion, accentuated curves of Spee and Wilson in the upper arch and reversed curves of Spee and Wilson in the lower arch, anterior spacing and diastema.
Treatment of endogenous tongue thrust is disputed. While retraining exercises may be employed, there may be additional tongue tissue present as well as subconscious activity. Partial glossectomy has been proposed as a possible adjuct to orthodontic treatment when tongue thrust or macroglossia is the main aetiology.16
This article presents the treatment of a 33-year-old woman of African descent with significant anterior open bite and macroglossia, who was treated with partial glossectomy and upper and lower pre-adjusted edgewise appliances.
Case report
Diagnosis and aetiology
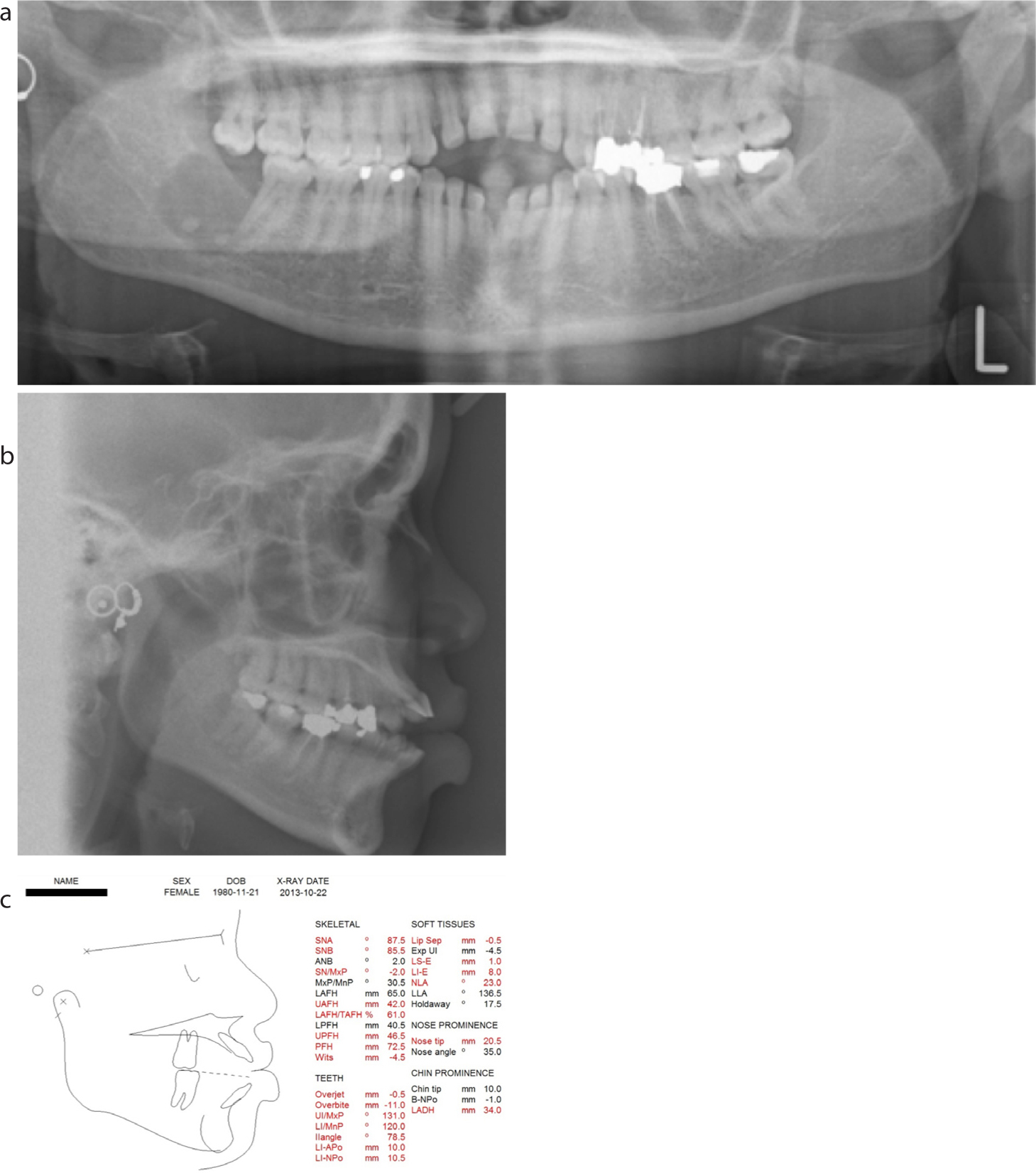
A fit and healthy 33-year-old female, originally from the Gambia, was referred to the Orthodontic department at the York Teaching Hospital by her general dental practitioner. She complained of an excessive anterior open bite, difficulty in eating and unsatisfactory appearance of her teeth. Periodontal status was sound with no pocket depth greater than 3 mm. On clinical examination she presented a mild Class III skeletal base and mildly increased vertical proportions.20 There was bimaxillary proclination with an anterior open bite of 11 mm and severe spacing in the upper and lower anterior segments. The molar relationships were Class I bilaterally, there was an increased curve of Spee in the upper arch and reversed curve of Spee in the lower arch. The upper lip length was normal at 23 mm, but there was no incisor show on smiling or at rest. The posterior dentition was heavily restored. The lower right third molar had previously been extracted and there was radiographic evidence of a small cystic lesion in the body of the mandible. There was relative macroglossia and the tongue was positioned anteriorly, sitting between the upper and lower teeth (Figure 1a-c). The main aetiology of the anterior open bite was thought to be the relative macroglossia and this was discussed with the patient at length.
Figure 1. (a–c) Pre-treatment radiographs and cephalometric tracing.
Treatment aims
Following review with an oral and maxillofacial surgeon, the following treatment aims were agreed:
Partial glossectomy (Obwegeser modification);
Attempt to reduce anterior open bite using fixed appliances only;
Maintain Class I molar relationships;
Permanent retention with bonded retainers.
Treatment alternatives
Should closure of the anterior open bite not be possible with orthodontic appliances only, a segmental anterior maxillary set down osteotomy, or three-part maxillary osteotomy would be performed following orthodonticpreparation.
Treatment progress
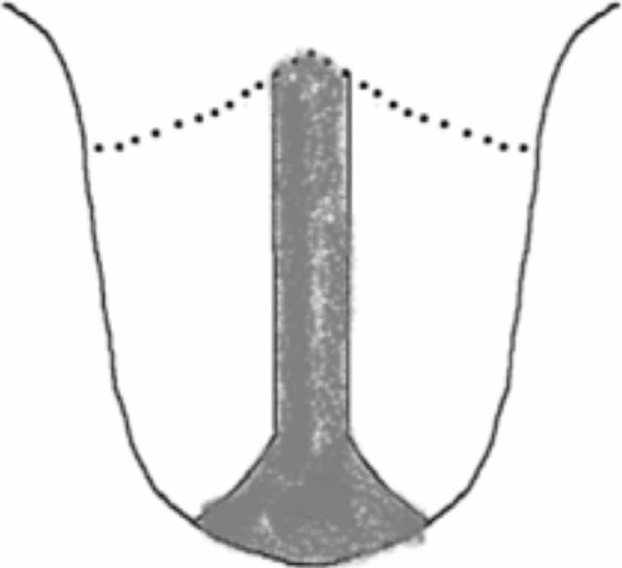
Treatment began with partial glossectomy under a general anaesthetic. There was full thickness resection of the tip of the tongue and partial thickness resection of the mid dorsum of the tongue (Figure 2) in conjunction with some laser ablation to the muscles. Closure was achieved with resorbable sutures. This tongue reduction design was chosen to reduce the length and width of the tongue21 while minimizing the risk of damage to the lingual and hypoglossal nerves in the ventral portion of the tongue. Healing occurred uneventfully, but an anterior tongue tie (ankoglossia) developed 8 weeks post-operatively and was released under local anaesthetic.
Figure 2. (a–h) Pre-treatment photographs.
Orthodontic treatment progressed using an 0.022” x 0.028” slot pre-adjusted edgewise system with MBT prescription. The heavily restored premolars on the left hand side were not bonded. Following the tongue reduction, the AOB had reduced to 9 mm. Levelling and alignment was completed using an 0.016” nickel–titanium (Ni–Ti) archwire, and 8 weeks later, retraction of the upper and lower labial segments was started using 0.018” stainless steel (SS) archwires, with tip back bends, bypassing the premolars and lacebacks in all four quadrants. Elastic powerchain was placed in the anterior segments, and treatment progressed with similar mechanics for 6 months with the aim of levelling the arches and extruding the incisors to improve incisal show (Figure 3).
Figure 3. Diagram of proposed partial glossectomy. Shaded area indicates removed tissue – full thickness tip of tongue and partial thickness mid-dorsum.
Anterior box elastics were worn (1/4”, 3.5 oz) to aid AOB closure for 4 months (Figure 4). Appliances were debonded and bonded and removable retainers with posterior bite blocks (active) were provided immediately. The total orthodontics treatment time was 14 months, 18 months including surgical time.
Figure 4. Anterior space closed after 6 months of active space closure.
Treatment results
The final occlusion was a well inter-digitated Class I with positive overbite. At the 1-year review, there had been some relapse of the AOB. However, this remained stable at 2 years post debond (Figure 5). There had been two episodes of the upper bonded retainer debonding from one tooth. At the 2-year review, new removable retainers were provided without bite blocks.
Figure 5. Anterior open-bite closed after 6 weeks of anterior elastics. Intermaxillary traction was continued to maintain change for 12 more weeks.
Discussion
The use of surgical tongue reduction in patients with macroglossia,16,19,22,23,24,25 endogenous tongue thrust, or those affected with Beckwith–Weidermann syndrome26 has been documented in the past. The predictability of treatment of an anterior open bite is reliant on sound diagnosis in the first instance and correction of the aetiological factor.
In the documented case report, the tongue, rather than skeletal abnormality, was felt to be the main aetiology and partial glossectomy considerably aided in the stability of the orthodontic correction. Should the anterior open bite not have been fully corrected with orthodontics alone, a segmental maxillary osteotomy was considered; however, this carries significant risks, including devitalization and loss of the maxillarysegment.27,28
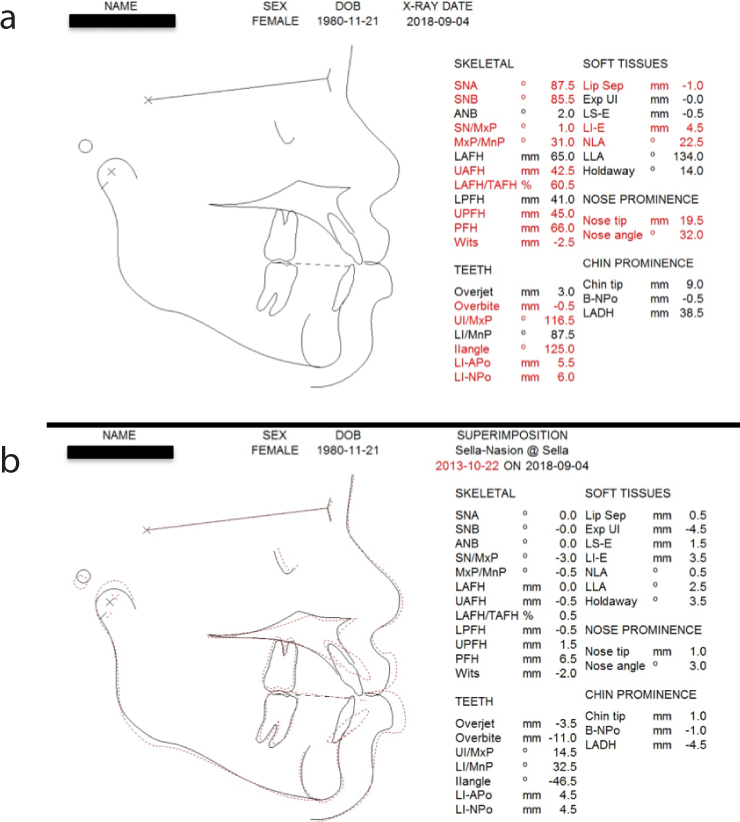
The cephalometric superimposition of pre- and post-treatment radiographs (Figure 6) demonstrates that the AOB has been closed by tipping and retraction of the upper and lower incisors with minimal mesial movement of the molars. The use of light forces to close anterior spacing has aided in prevention of loss of anchorage, especially because, following the partial glossectomy, there was a reduction in soft tissue forces resisting retraction.29
Figure 6. (a–h) Two-year follow up post debond. AOB reduction has remained relatively stable following treatment.
The patient has not reported any significant problems following her partial glossectomy and, apart from the mild anterior tongue tie that developed, has had no complications. At the final review, the patient did mention a slight ‘heavy feeling’ in the tongue and was advised to have haematinic analysis with her general medical practitioner. Sensory changes following tongue reduction have been reported,30 with changes in the threshold for taste and pain perception in the short term following surgery;31 however, other studies have found no differences in taste perception following tongue reduction in patients with Beckwith–Weidermann syndrome.32
The smile aesthetics and incisor show have dramatically improved following orthodontic treatment, and this combined with good occlusal result, shows an excellent treatment strategy despite some mild relapse of the AOB following appliance removal.
Conclusions
This is a case report documenting the treatment of a significant anterior open bite associated with macroglossia. An Obwegeser modification partial glossectomy aided orthodontic treatment and contributed to the stability, at least in the medium term (2 years post debond), of the post-treatment result.
Figure 7. (a, b) Post-treatment cephalometric tracing and superimposition.