Brezniak N, Wasserstein A Orthodontically induced inflammatory root resorption. Part I: The basic science aspects. Angle Orthod. 2002; 72:(2)175-179
Kaley J, Phillips C Factors related to root resorption in edgewise practice. Angle Orthod. 1991; 61:(2)125-132
Brin I, Tulloch JF, Koroluk L, Philips C External apical root resorption in Class II malocclusion: a retrospective review of 1-versus 2-phase treatment. Am J Orthod Dentofacial Orthop. 2003; 124:(2)151-156
Brudvik P, Rygh P Root resorption beneath the main hyalinized zone. Eur J Orthod. 1994; 16:(4)249-263
Chan E, Darendeliler MA Physical properties of root cementum: part 7. Extent of root resorption under areas of compression and tension. Am J Orthod Dentofacial Orthop. 2006; 129:(4)504-510
Han G, Huang S, Von den Hoff JW, Zeng X, Kuijpers-Jagtman AM Root resorption after orthodontic intrusion and extrusion: an intraindividual study. Angle Orthod. 2005; 75:(6)912-918
Harris DA, Jones AS, Darendeliler MA Physical properties of root cementum: part 8. Volumetric analysis of root resorption craters after application of controlled intrusive light and heavy orthodontic forces: a microcomputed tomography scan study. Am J Orthod Dentofacial Orthop. 2006; 130:(5)639-647
Jimenez-Pellegrin C, Arana-Chavez VE Root resorption in human mandibular first premolars after rotation as detected by scanning electron microscopy. Am J Orthod Dentofacial Orthop. 2004; 126:(2)178-184
Parker RJ, Harris EF Directions of orthodontic tooth movements associated with external apical root resorption of the maxillary central incisor. Am J Orthod Dentofacial Orthop. 1998; 114:(6)677-683
Sameshima GT, Sinclair PM Predicting and preventing root resorption: Part II. Treatment factors. Am J Orthod Dentofacial Orthop. 2001; 119:(5)511-515
Owman-Moll P, Kurol J, Lundgren D Continuous versus interrupted continuous orthodontic force related to early tooth movement and root resorption. Angle Orthod. 1995; 65:(6)395-401
Weiland F Constant versus dissipating forces in orthodontics: the effect on initial tooth movement and root resorption. Eur J Orthod. 2003; 25:(4)335-342
Miura F, Mogi M, Ohura Y, Hamanaka H The super-elastic property of the Japanese NiTi alloy wire for use in orthodontics. Am J Orthod Dentofacial Orthop. 1986; 90:(1)1-10
Mandall N, Lowe C, Worthington H, Sandler J, Derwent S, Abdi-Oskouei M Which orthodontic archwire sequence? A randomized clinical trial. Eur J Orthod. 2006; 28:(6)561-566
Mavragani M, Vergari A, Selliseth NJ, Boe OE, Wisth PL A radiographic comparison of apical root resorption after orthodontic treatment with a standard edgewise and a straight-wire edgewise technique. Eur J Orthod. 2000; 22:(6)665-674
Scott P, DiBiase AT, Sherriff M, Cobourne MT Alignment efficiency of Damon3 self-ligating and conventional orthodontic bracket systems: a randomized clinical trial. Am J Orthod Dentofacial Orthop. 2008; 134:(4)470-e8
Pandis N, Nasika M, Polychronopoulou A, Eliades T External apical root resorption in patients treated with conventional and self-ligating brackets. Am J Orthod Dentofacial Orthop. 2008; 134:(5)646-651
Fritz U, Diedrich P, Wiechmann D Apical root resorption after lingual orthodontic therapy. J Orofac Orthop. 2003; 64:(6)434-442
Brezniak N, Wasserstein A Root resorption following treatment with aligners. Angle Orthod. 2008; 78:(6)1119-1124
Barbagallo LJ, Jones AS, Petocz P, Darendeliler MA Physical properties of root cementum: Part 10. Comparison of the effects of invisible removable thermoplastic appliances with light and heavy orthodontic forces on premolar cementum. A microcomputed-tomography study. Am J Orthod Dentofacial Orthop. 2008; 133:(2)218-227
Smith NJ Orthodontic radiology: a review. Int Dent J. 1987; 37:(1)16-24
McNicol A, Stirrups DR Radiation dose during the dental radiographic techniques most frequently used during orthodontic treatment. Eur J Orthod. 1985; 7:(3)163-171
Ferguson JW, Evans RI, Cheng LH Diagnostic accuracy and observer performance in the diagnosis of abnormalities in the anterior maxilla: a comparison of panoramic with intraoral radiography. Br Dent J. 1992; 173:(8)265-271
Leach HA, Ireland AJ, Whaites EJ Radiographic diagnosis of root resorption in relation to orthodontics. Br Dent J. 2001; 190:(1)16-22
Årtun J, Van't Hullenaar R, Doppel D, Kuijpers-Jagtman AM Identification of orthodontic patients at risk of severe apical root resorption. Am J Orthod Dentofacial Orthop. 2009; 135:(4)448-455
da Silveira HL, Silveira HE, Liedke GS, Lermen CA, Dos Santos RB, de Figueiredo JA Diagnostic ability of computed tomography to evaluate external root resorption in vitro. Dentomaxillofac Radiol. 2007; 36:(7)393-396
Dudic A, Giannopoulou C, Leuzinger M, Kiliaridis S Detection of apical root resorption after orthodontic treatment by using panoramic radiography and cone-beam computed tomography of super-high resolution. Am J Orthod Dentofacial Orthop. 2009; 135:(4)434-437
Remington DN, Joondeph DR, Årtun J, Riedel RA, Chapko MK Long-term evaluation of root resorption occurring during orthodontic treatment. Am J Orthod Dentofacial Orthop. 1989; 96:(1)43-46
Levander E, Malmgren O Long-term follow-up of maxillary incisors with severe apical root resorption. Eur J Orthod. 2000; 22:(1)85-92
Kalkwarf KL, Krejci RF, Pao YC Effect of apical root resorption on periodontal support. J Prosthet Dent. 1986; 56:(3)317-319
Levander E, Malmgren O, Eliasson S Evaluation of root resorption in relation to two orthodontic treatment regimes. A clinical experimental study. Eur J Orthod. 1994; 16:(3)223-228
George A, Evans CA Detection of root resorption using dentin and bone markers. Orthod Craniofac Res. 2009; 12:(3)229-235
Putranto R, Oba Y, Kaneko K, Shioyasono A, Moriyama K Effects of bisphosphonates on root resorption and cytokine expression during experimental tooth movement in rats. Orthodontic Waves. 2008; 67:141-149
Talic NF, Evans C, Zaki AM Inhibition of orthodontically induced root resorption with echistatin, an RGD-containing peptide. Am J Orthod Dentofacial Orthop. 2006; 129:(2)252-260
El-Bialy T, El-Shamy I, Graber TM Repair of orthodontically induced root resorption by ultrasound in humans. Am J Orthod Dentofacial Orthop. 2004; 126:(2)186-193
Årtun J, Smale I, Behbehani F, Doppel D, Van't Hof M, Kuijpers-Jagtman AM Apical root resorption six and 12 months after initiation of fixed orthodontic appliance therapy. Angle Orthod. 2005; 75:(6)919-926
The aim of this second article in this series of two is to outline the treatment-related factors, which are understood to play an important role in orthodontically-induced inflammatory root resorption (OIIRR). This article will highlight the importance of patient assessment, as well as the long-term effects of OIIRR. It will also discuss future developments, which may improve our understanding of the mechanisms of tooth movement and root resorption.
Clinical Relevance: The orthodontic practitioner should be aware of the iatrogenic effects of treatment mechanics and the need for detailed patient assessment prior to the start of treatment to reduce harmful consequences.
Article
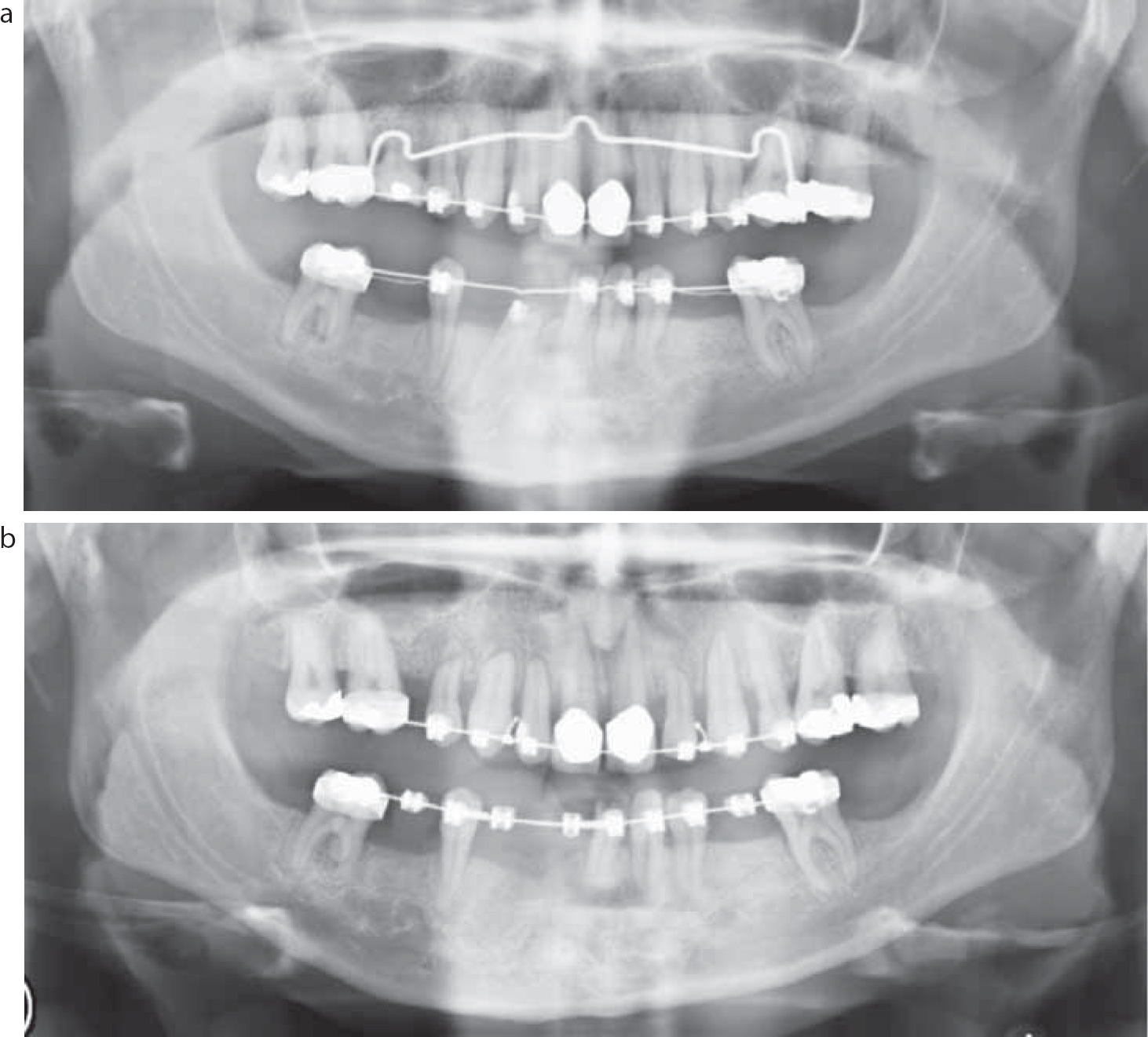
Orthodontically-induced inflammatory root resorption (OIIRR) occurs when orthodontic forces are applied to the dentition (Figure 1). This results in the induction of a local periodontal inflammatory process. This inflammation, which is essential for tooth movement, is the fundamental component of the root resorption process and causes remodelling of both cementum and dentine of the roots.1 During periods of relative quiescence, the cementum undergoes repair such that, for most teeth in most patients, the changes in root length are so small as to be difficult to detect and are often clinically insignificant.2 Different treatment modalities have been implicated in the development of OIIRR and the extent to which this affects the dentition.
Figure 1. Root resorption during orthodontic treatment: (a) initial alignment; (b) stainless steel archwires (courtesy of Mr Christian Day).
Treatment factors
Duration of treatment
Although there is not a large body of evidence linking the length of treatment to an increased risk of root resorption, Brin et al3 examined the effect of 2-phase vs 1-phase treatment of Class II cases on root resorption. They suggested that those children who underwent a 2-phase treatment, using a Bionator functional appliance followed by fixed appliances, had the fewest incisors with moderate to severe OIIRR. They also demonstrated that, as treatment time increased, so did the odds of OIIRR. The odds of a tooth experiencing severe root resorption were greater with a large reduction in overjet during phase 2.
Magnitude of force
It has been suggested that high levels of force will increase the damaged areas in the periodontal ligament, which may lead to more extensive OIIRR.4 This has been supported by more recent studies. Chan and Darendeliler5 found that heavy forces produced significantly more root resorption than light forces or controls. Their studies showed that the mean volume of resorption craters was nearly 12 times greater in the heavy force group than in the control group who had not undergone orthodontic treatment. In conclusion, there is a body of evidence to suggest that heavy forces could be particularly damaging.
Types of tooth movement
Studies using scanning electron microscopy have revealed that root resorption is not only dependent upon time taken and force used, but also the type of tooth movement to which the teeth are subjected. Han et al found that intrusion of teeth caused about four times more root resorption than extrusion.6
Further examination of the magnitude of intrusive forces showed that light intrusive forces (25 g) produced twice the volume of resorption compared to controls, and that heavy forces (225 g) increased the volume of resorption by a factor of 4.7
Rotational correction has also been shown to increase root resorption, but the areas affected are mainly in the medial third of the roots and correspond to the most prominent regions on the root surface.8 Previously, this has largely gone undetected, as standard radiological techniques would fail to provide information on the three-dimensional architecture of the teeth.
When examining the maxillary central incisors, movements that torque the apex lingually are strongly correlated with root resorption.9 Kaley and Phillips reported a 20-fold increase in the risk of severe root resorption of the maxillary incisors if their roots were forced against the lingual cortical plate.2
Extraction patterns
The literature is inconclusive on whether the extraction pattern affects the extent of OIIRR. Sameshima and Sinclair10 concluded that extraction of premolars increased the amount of root resorption compared to non-extraction treatment. This may arise due to greater distances of tooth movement seen where teeth are extracted. Interestingly, patients who had extraction of upper first premolars had no significant differences with the non-extraction group. This would seem to contradict any theories relating to the amount of tooth movement being correlated with increased root resorption, as correction of an increased overjet is likely to increase the forces on the upper labial segment and thus increase root resorption.
Continuous vs discontinuous force
From a cost-benefit point of view, orthodontic treatment should be performed as quickly as possible and with minimal damage to the surrounding tissues. The study by Owman-Moll et al11 demonstrated that tooth movements were achieved more effectively with the use of continuous forces.
However, it is believed that discontinuous forces allow for periods of rest which favourably affect cell proliferation in the supporting tissues. In these rest periods, the resorption cavities are repaired with secondary cementum. In a split-mouth design investigation, Owman- Moll et al11 did not find any difference in the amount and severity of root resorption between continuous and interrupted forces.
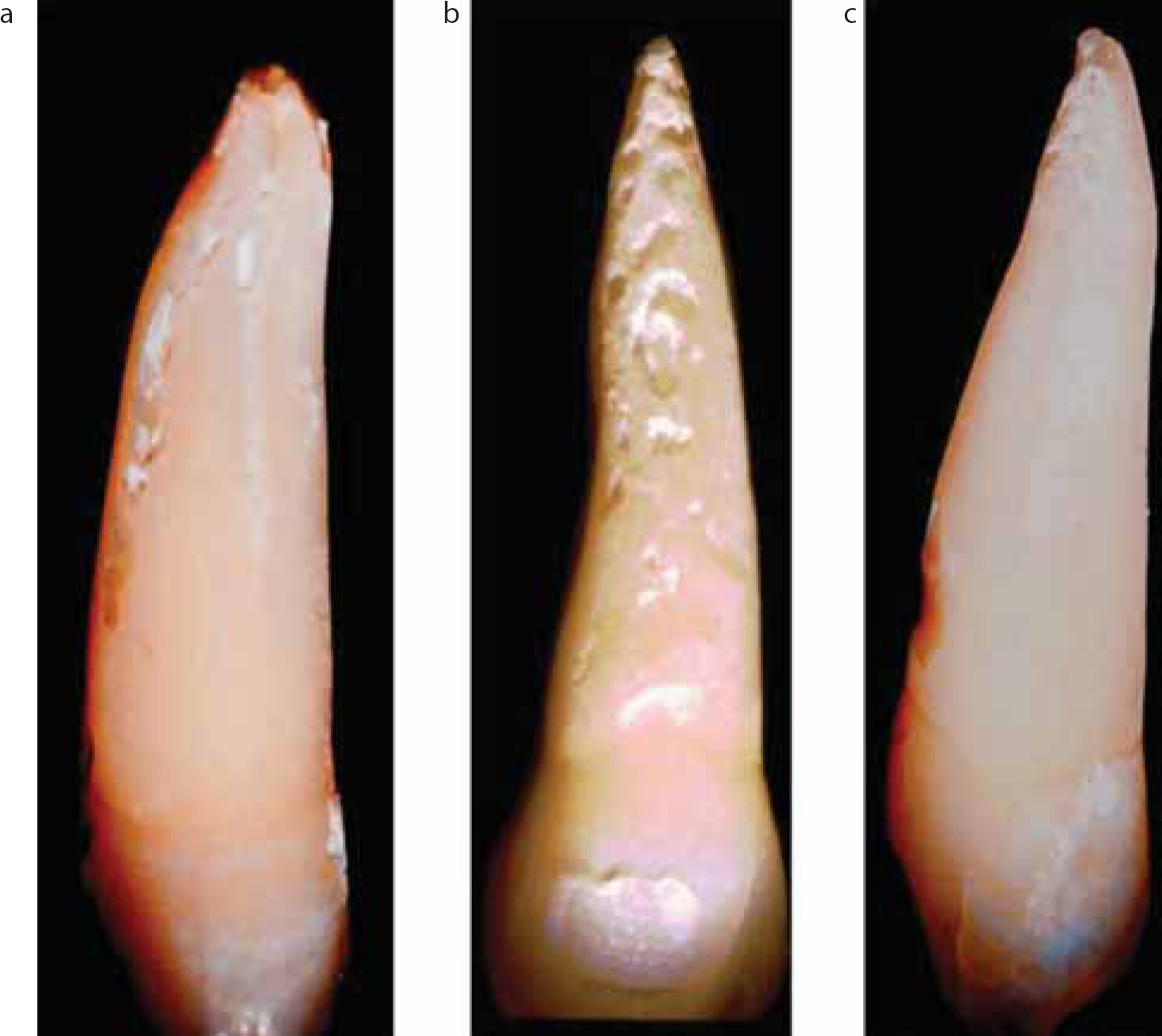
Their explanation was that the frequency and duration of the rest periods required within an interrupted force system, that are necessary to minimize root resorption and yet maintain treatment efficiency, remain unclear. Weiland12 found that there was a significant increase in the area and volume of the resorption lacunae on the roots that were moved with superelastic nickel titanium wires compared to those moved with stainless steel wires. Super-elastic wires deliver a constant force over an extended portion of the deactivation range, whereas stainless steel wires produce an initial high level of force which declines rapidly (Figure 2).13
Figure 2.
(a, b) Continuous orthodontic movement with nickel titanium archwire and (c) intermittent orthodontic tooth movement with stainless steel archwires. All teeth extracted after three months' movement (a and c courtesy of Dr F Weiland; b reprinted from Kontinuierliche versus nicht-kontinuierliche Kraefte in der Kieferorthopaedie with the kind permission of Quintessenz Verlags-GmbH, Berlin).
Archwire sequence
Mandall et al14 reported a randomized clinical trial investigating the effect of three archwire sequences on patient discomfort, root resorption and time to working archwire. They concluded that there was no statistically significant difference between the proportion of patients with or without root resorption in the three groups. They accepted that this study may have underestimated root resorption, as the data only recorded up to passive placement of working archwires and not to the end of treatment.
Orthodontic appliances
Many manufacturers claim that their appliances produce less friction and thus less force to move teeth. This would logically translate to the possibility of less root resorption with reduced forces being applied to the periodontal tissues. Comparisons between different appliance systems have found differing results (Figure 3). Mavragani et al15 compared conventional edgewise with the straight-wire technique, finding increased levels of root resorption on the incisors with the edge-wise technique, although the groups may have not been entirely matched for overjet.
Scott et al16 undertook a randomized clinical trial of two bracket systems: one group of patients was treated with Damon3 self-ligating brackets and the second group with pre-adjusted edgewise brackets. Their study failed to find any statistical difference between a self-ligating and conventional orthodontic bracket system and root resorption. This was confirmed by Pandis et al,17 comparing conventional edgewise appliance with Damon2, who found no statistical differences in OIIRR between the two groups.
Fritz et al,18 albeit with a small sample of patients treated with lingual appliances, found similar results to those for conventional labial appliances.
Although there is limited evidence regarding other treatment methods, a recent case report showed extensive root resorption from Invisalign aligner therapy.19 The aligner is essentially a removable appliance that provides intermittent forces to the teeth with movement of around 0.2 to 0.5 mm per aligner. In a split mouth experiment of OIIRR caused by thermoplastic appliances (aligners), light forces (25 g) and heavy forces (225 g), the authors showed a 6-fold increase in root resorption with aligners, 5-fold increase with light forces and a 9-fold increase with heavy forces, compared to controls.20 Thus the aligner can be considered to apply similar forces to light forces used with fixed appliances.
Patient assessment
Before starting a course of orthodontic treatment, a full clinical and radiographic examination should be undertaken and teeth which are abnormally mobile or have had a history of trauma must be identified.
Radiographs are usually taken to assess general dental health, including root form and the presence or absence of any underlying disease, and to show the position and number of developing teeth (Figure 4).21 A view which is generally regarded to be the most useful for these purposes is the dental panoramic tomogram (DPT). It subjects the patient to a lower dose of radiation than a series of full-mouth intra-oral radiographs, yet supplies the clinician with an overall view of the dentition.22
Figure 4. Cephalometric radiograph highlighting its use in assessment of root length.
However, because the focal trough of the tomographic view is narrow in the incisor region, the apices of the teeth and any associated palatal structures in this region can be out of focus or even invisible. Therefore, intra-oral views are recommended, in addition to the DPT, when there is an indication of an underlying anomaly or pathology.23 According to Leach et al,24 intra-oral radiographs should be geometrically accurate and reproducible, especially if root resorption is to be assessed over time. For these reasons, they recommend the long cone paralleling technique rather than the bisected angle technique. They explain that the bisecting angle technique often leads to foreshortening or elongation of the teeth in the final image. The upper standard occlusal radiograph is, in effect, a large bisected angle technique radiograph, so subject to the same disadvantages and distortions.
The use of digital radiography allows manipulation of the image in terms of enlargement, contrast enhancement and inversion, which may improve the assessment of root resorption. Geometric errors may still arise if a long cone paralleling technique is used and the image can still be subjected to magnification and projection errors of around 2 mm.25 This makes the assessment of the severity of OIIRR very difficult as, in most cases, OIIRR is around 2 mm. Årtun et al suggested a method which reduced the enlargement to 0.7 mm by reconstructing the radiographic image based on anatomical landmarks of the initial radiograph.25 Alternatives have been described by the use of a 9 mm metal wire placed parallel to the crown.6
In the future, investigative procedures, such a cone-beam computed tomography (CBCT), may add much to our knowledge and subsequent management of root resorption. CBCT is a low dose scanning system which has the ability to provide a three-dimensional image of the roots. In vitro studies have demonstrated that CBCT's diagnostic ability of root resorption showed high sensitivity and excellent specificity.26
Comparisons between dental panoramic Tomograms (DPT) and CBCT's ability to discern EARR have shown the underestimation of EARR on DPTs. Dudic et al found that 56.5% and 31% of teeth evaluated showed no resorption by DPT and CBCT, respectively, 33.5% and 49% showing mild resorption, 8% and 19% showed moderate resorption and only the CBCT showed severe resorption in two teeth. It also highlighted the inherent problems with the DPT when assessing the anterior teeth, with 16% of teeth being unable to be evaluated.27 As root resorption is a three-dimensional phenomenon, the use of two-dimensional radiography will always underestimate the severity of the problem.
Long-term effects of root resorption
Our understanding is that root resorption stops after active treatment.28 Even extensive root resorption does not usually affect the functional capacity or greatly compromise the longevity of the teeth. From their study of 100 patients recalled on average 14 years after orthodontic treatment, Remington et al28 found tooth loss and hyper-mobility in only two cases.
This is emphasized by a more recent retrospective study of patients with severe root resorption who were reviewed 5 to 15 years after treatment. This study found that no teeth were abnormally mobile and none had been lost.29
Significant root loss will cause an unfavourable crown-root ratio of the affected teeth, making these teeth less suitable as abutments for prosthetic restorations. Apical root loss of 3 mm is equivalent to 1 mm of crestal bone loss, so periodontitis will progress more rapidly to a critical alveolar bone level if it involves teeth with root resorption.30
It is widely accepted that, if severe root resorption is identified during treatment, the patient must be informed and the treatment plan reassessed. There is some evidence that a 2 to 3 month treatment pause decreases further root resorption.31
Future developments
Advances in molecular biology have improved our understanding of the mechanisms of tooth movement at the cellular level. Changes in the composition of gingival crevicular fluid (GCF)32 offer a potential method of determining if root resorption can be detected from differences in the concentrations of bone and dentine markers. The use of GCF has many advantages in that it is relatively non- invasive and may provide more sensitive information on root resorption without the inherent flaws in two-dimensional radiography and the increased doses of three-dimensional CBCT. Further work is needed into this area of research to elucidate any correlations between these markers and the potential for root resorption. Some preliminary results from studies in animals, investigating the use of chemical agents such as bisphosphonates33 and echistatin,34 have found a reduction in the rate of root resorption by targeting osteoclast receptors. Conversely, these agents also reduce bone turnover and thus orthodontic tooth movement.
Treatment of root resorption has been demonstrated to be effective by the use of low intensity pulsed ultrasound.35 This causes hypercementosis and healing of the root surface. Further work is needed to elucidate any possible clinical applications of this technique.
Conclusion
So what can we conclude from the studies on root resorption to date? It would appear that individual variation makes it difficult to predict the likelihood or extent of root resorption that might arise as a result of orthodontic treatment. However, there is a body of evidence to suggest that orthodontic treatment does increase the incidence of root resorption, and that heavy forces could be particularly damaging to teeth in this respect. Patients who have sustained OIIRR in the first six months of treatment are more likely to experience further root resorption in the subsequent six months compared to patients that have shown no evidence of root resorption.36 There is no evidence that OIIRR is affected by bracket systems or archwire sequencing, although there is some evidence that super-elastic archwires, through their continuous range of activity, can induce greater levels of root resorption.12
It is therefore important to try and identify those factors which might contribute to root resorption in order to minimize their potential effect and patients must be advised of the risk of root resorption before starting treatment, as part of the process of informed consent.