Van Meerbeek B, Inoue S, Perdiago J, Lambrechts P, Vanherle G Enamel in dentine adhesion, 2nd edn. London: Quintessence Publishing; 2001
Miller RA Laboratory and clinical evaluation of a self-etching primer. J Clin Orthod. 2001; 35:42-45
Chu CH, Ou KL, Dong de R Orthodontic bonding with self-etching primer and self-adhesive systems. Eur J Orthod. 2011; 33:276-281
Fleming PS, Johal A, Pandis N Self-etch primers and conventional acid-etch technique for orthodontic bonding: a systematic review and meta-analysis. Am J Orthod Dentofacial Orthop. 2012; 142:83-94
Grewal Bach GK, Torrealba Y, Lagravère MO Orthodontic bonding to porcelain: a systematic review. Angle Orthod. 2014; 84:555-560
Shenoy A, Shenoy N Dental ceramics: an update. J Conserv Dent. 2010; 13:195-203
Karan S, Toroglu MS Porcelain refinishing with two different polishing systems after orthodontic debonding. Angle Orthod. 2008; 78:947-953
Costa AR, Correr AB, Puppin-Rontani RM Effect of bonding material, etching time and silane on the bond strength of metallic orthodontic brackets to ceramic. Braz Dent J. 2012; 23:223-227
Barceló Santana HF Evaluation of bond strength of metal brackets by a resin to ceramic surfaces. J Clin Dent. 2006; 17:5-9
Eslamian L, Ghassemi A, Amini F, Jafari A, Afrand M Should silane coupling agents be used when bonding brackets to composite restorations? An in vitro study. Eur J Orthod. 2009; 232:274-280
Pannes DD, Bailey DK, Thompson JY, Pietz DM Orthodontic bonding to porcelain: a comparison of bonding systems. J Pros Dent. 2003; 89:66-69
Keim RG, Gottlieb EL, Nelson AH, Vogels DS JCO Study of orthodontic diagnosis and treatment procedures, part 1. Results and trends. J Clin Orthod. 2002; 36:553-568
Zachrisson BU Orthodontic bonding to artificial tooth surfaces: clincial versus laboratory findings. Am J Orthod Dentofacial Orthop. 2000; 117:592-594
Buyukyilmaz T, Zachrisson B Improved orthodontic bonding to silver amalgam. Part 2. Lathe-cut, admixed, and spherical amalgams with different intermediate resins. Angle Orthod. 1998; 68:337-344
Jost-Brinkmann PG, Bohme A Shear bond strengths attained in vitro with light-cured glass ionomers vs composite adhesives in bonding ceramic brackets to metal or porcelain. J Adhes Dent. 1999; 1:243-253
Zachrisson BU, Buyukyilmaz T Recent advances in bonding to gold, amalgam and porcelain. J Clin Orthod. 1993; 27:661-675
Zachrisson BU, Buyukyilmaz T, Zachrisson YO Improving orthodontic bonding to silver amalgam. Angle Orthod. 1995; 65:35-42
Setcos JC, Staninec M, Wilson NHF The development of resin bonding for amalgam restorations. Br Dent J. 1999; 186:328-332
Pimentel AH, Valente LL, Isolan CP Effect of waiting time for placing resin composite restorations after bleaching on enamel bond strength. Appl Adhes Sci. 2015; 3:(23)
McEvoy SA Chemical agents for removing intrinsic stains from vital teeth. Part II. Current techniques and their clinical application. Quintessence Int. 1989; 20:379-384
Titley KC, Torneck CD, Smith DC, Adibfar A Adhesion of composite resin to bleached and unbleached bovine enamel. J Dent Res. 1988; 67:1523-1528
Nour El-din AK, Miller BH, Griggs JA, Wakeld C Immediate bonding to bleached enamel. Oper Dent. 2006; 31:106-114
Gurgan S, Alpaslan T, Kiremitci A, Cakir FY Effect of different adhesive systems and laser treatment on the shear bond strength of bleached enamel. J Dent. 2009; 37:527-534
Moule CA, Angelis F, Kim GH, Le S Resin bonding using an all-etch or self-etch adhesive to enamel after carbamide peroxide and/or CPP-ACP treatment. Aust Dent J. 2007; 52:133-137
Noble J, Karaiskos NE, Wiltshire WA In vivo bonding of orthodontic brackets to fluorosed enamel using an adhesion promotor. Angle Orthod. 2008; 78:357-360
Hoffman S, Royelstad R, McEwan WS, Drew CM Demineralisation studies of fluoride treated enamel using scanning electron microscopy. J Dent Res. 1969; 48:1296-1302
Kochavi D, Gedalia I, Anaise J Effects of conditioning with fluoride and phosphoric acid on enamel surfaces as evaluated by scanning electron microscopy and fluoride incorporation. J Dent Res. 1975; 54:304-309
Opinya GN, Pameijer CH Tensile bond strength of fluorosed Kenyan teeth using the acid etch technique. Int Dental J. 1986; 336:225-229
Miller RA Bonding fluorosed teeth: new materials for old problems. J Clin Orthod. 1995; 29:424-427
Ng'ang'a PM, Ogaard B, Cruz R Tensile strength of orthodontic brackets bonded to fluorotic and nonfluorotic teeth: an in vitro comparative study. Am J Orthod Dentofacial Orthop. 1992; 102:244-250
Seymen F, Kiziltan B Amelogenesis imperfecta: a scanning electron microscopic and histopathalogic study. J Clin Pediatr Dent. 2002; 26:327-335
Arkutu N, Gadhia K, McDonald S, Malik K, Currie L Amelogenesis imperfecta: the orthodontic perspective. Br Dent J. 2012; 212:485-489
Seow W, Amaratunge A The effects of acid etching on enamel from different clinical variants of amelogenesis imperfecta: an SEM study. Pediatr Dent. 1998; 20:37-42
Orthodontic bonding techniques continue to evolve with the ever-changing population. With the demand for orthodontic treatment increasing, the specialty is regularly presented with restored dentitions, anterior crowns, bleached teeth, as well as those presenting with developmental conditions, such as fluorosis and amelogenesis imperfecta. Reduced orthodontic bond strength can lead to failure of the appliance and in turn lead to prolonged treatment times and patient dissatisfaction. This article aims to summarize the recommended methods for bonding and give an updated review of optimizing techniques.
CPD/Clinical Relevance: Adequate bracket bond strength is an essential part of orthodontic treatment, to prevent breakages and reduce treatment time and risk factors.
Article
Naomi Prado
The invention of direct bonding of brackets to enamel surfaces of teeth has dramatically changed orthodontic treatment. The acid-etch bonding technique was introduced by Buonocore in 19551 and later adopted by Newman for the attachment of orthodontic brackets.2 This led to the progression from the traditional banding of individual teeth, to the direct bonding technique that is now ubiquitous.
This ability to bond orthodontic brackets directly has offered numerous clinical advantages including: reduced patient chair-time; increased patient comfort; improved aesthetics; reduced plaque retention; and the possibility of placing attachments on partially erupted teeth.
Although a number of bonding materials have been trialled, composite has been found to be the most effective for orthodontic bonding, exhibiting adequate bond strength to withstand intra-oral and orthodontic forces (6−8 MPa at 24 hours,3 with acceptable bond failure rate of 1−5%4). With the demand for orthodontic treatment increasing, particularly amongst the adult population, the specialty is facing new challenges. Many patients now present with teeth restored with a variety of materials, such as composite or amalgam fillings, porcelain veneers and ceramic or metal crowns. In an unrestored dentition, patients may also present with previously bleached teeth and both adult and adolescent patients may present with other atypical tooth surfaces, including developmental conditions such as fluorosis and amelogenesis imperfecta.
Many studies have reported different methods for optimizing bonding to these atypical surfaces and this article aims to discuss and summarize the most popular techniques.
Traditional acid-etch technique
Orthodontic bonding to enamel and dentine surfaces is done via the acid-etch technique, with composite resin.
An organic resin matrix (Bis-GMA, with a TEGDMA diluent to reduce viscosity);
Inorganic filler particles (commonly silica or glass-containing aluminium);
Initiators and accelerators (Camphorquinone);
Pigment for colour (usually metal oxides such as titanium or aluminium oxides).
Enamel is a highly mineralized tissue, made up of hydroxyapatite crystals (86%) with water and inorganic content.5 The hydroxyapatite crystals are arranged in rods with a smooth surface.
Bonding of composite resin to enamel is micromechanical in nature.6 The enamel surface is etched with 37% phosphoric acid, allowing selective dissolution of enamel rods and the creation of microporosities of around 30 micrometres in depth. A low viscosity resin (bond) is then applied, which penetrates into the microporosities and leads to the formation of resin tags.5 The resin tags allow micromechanical retention to the composite, which is light-cured (using blue light of 470 nm) to initiate free radical polymerization; thus changing the composite resin from a fluid to a solid state.5
In recent years, there has been a move towards simplifying the acid-etch technique, such as with the use of self-etching primers. These combine the conditioning (etch) and priming (bond) steps, therefore reducing clinical chair-time and the possibility of moisture contamination.7 The active ingredient in these products is methacrylated phosphoric acid ester, which dissolves calcium from the hydroxyapatite crystals in enamel. The calcium then attaches to the phosphate group of the ester and forms a complex, which is polymerized when the resin is set.8
A meta-analysis was conducted by Fleming et al in 2012, to review the evidence comparing bonding with traditional acid-etch technique, compared to using self-etching primers. The analysis concluded that there was no significant evidence to favour one system over the other, in terms of bond failure and reducing clinical chair-time.9 Therefore, the choice of methods for bonding to enamel is very much at the discretion of the operator.
Bonding to porcelain and ceramic surfaces
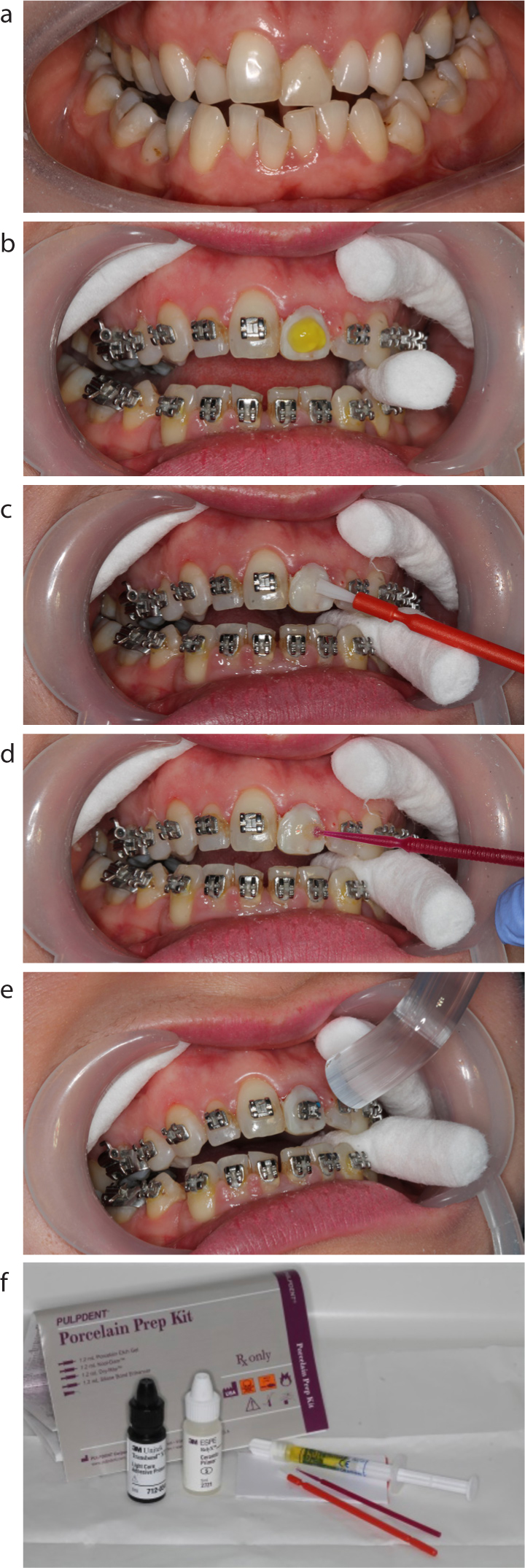
Bonding of orthodontic brackets to porcelain or ceramic surfaces exhibits a higher degree of failure, when compared to enamel.10 Dental porcelain/ceramics are glass materials with an amorphous structure containing metal oxides (silica/alumina).11 The most well recognized technique for bonding to porcelain is via the use of hydrofluoric acid and a silane coupling agent (Figure 1).
Figure 1.
(a−f) Steps for bonding to porcelain surfaces. (a) Patient presenting for bond-up with porcelain crown UL1. (b) Surface conditioning using simple diamond bur preparation and etch stage (for 60 seconds): note the soft tissue protection. (c) Application of a saline coupling agent. (d) Application of bond. (e) Placement of orthodontic bracket and light curing for polymerization. (f) Porcelain bonding kit (other manufacturers available).
Hydrofluoric acid (9.6%) has been shown to react with the silica phase within the porcelain, creating microchannels and so facilitating micromechanical retention.10 It has been found that longer etching time results in further dissolution of the glassy matrix and subsequent increase in overall surface area, by increased formation of the microchannels. For this reason, it is suggested that the etching phase of bonding is extended to 60 seconds.12 It is important to note that hydrofluoric acid is highly irritant to soft tissues and so extreme care and effective isolation should be exercised in clinical practice, to avoid acid burn of the surrounding tissues. High volume suction throughout the procedure is often recommended.
Multiple studies have found that the bond strength of orthodontic brackets to porcelain surfaces is significantly improved by the application of a silane coupling agent.13,14,15 Silane works by forming weak chemical bonds with both organic and inorganic surfaces, therefore bonding with both the porcelain surface and the composite resin.
In addition to the above steps, bond strengths can be further increased by mechanical surface conditioning procedures. The purpose of these techniques is to increase the surface area available for the bonding techniques to be successful as follows:
Diamond bur − the most widely available and easiest chair-side method is simple roughening of the porcelain by using a high-speed diamond bur to remove the glazed surface.
Sandblasting − chairside sandblasting with aluminium oxide particles to create irregularities in the porcelain surface.
Prior to any preparation of porcelain/ceramic surfaces for orthodontic bonding, patients should be informed and consented for the common risk that the restored surface will not be aesthetically uniform following debond. Even without additional surface conditioning (diamond bur or sandblasting) studies have shown that the restorations are often irreversibly damaged.16 Therefore, replacement of the restorations affected may be required, after the orthodontic appliances are removed. Fully informed consent for this stage must be obtained at the start of treatment.
Bonding to amalgam and metals
A study by Keim et al concluded that there had been a significant reduction in the number of orthodontists banding posterior teeth and, due to the advances in bonding, more clinicians were favouring bonding tubes onto molars.17 However, with the corresponding increase in numbers of the adult population undergoing orthodontic treatment, patients may present for treatment with extremely large amalgam restorations, often extending onto the buccal surfaces of their posterior teeth.
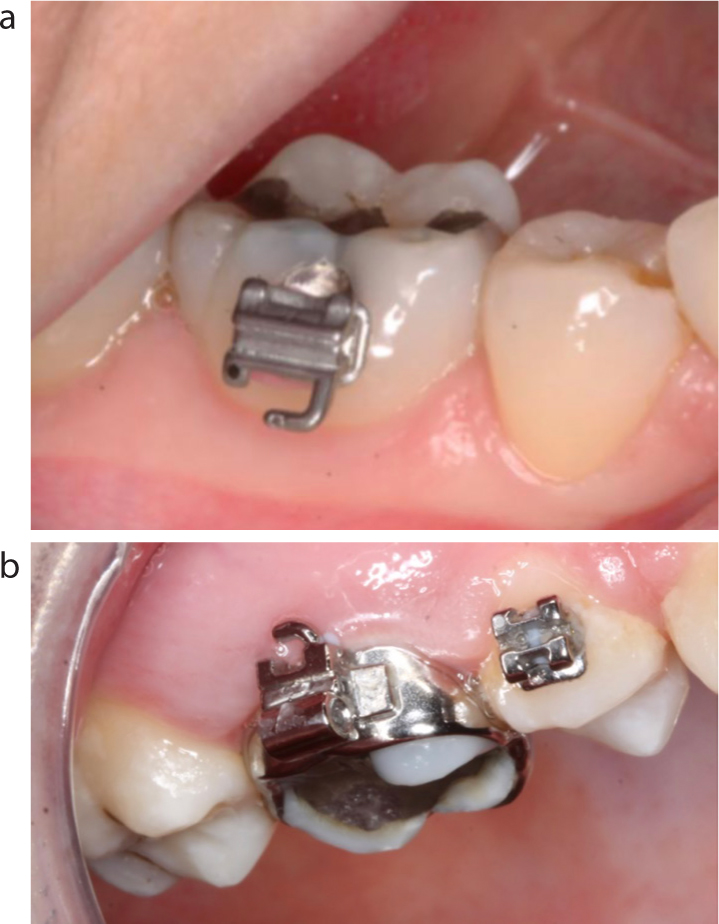
If the size of amalgam restoration is such that there is still significant adjacent tooth structure, then bonding via the conventional acid-etch technique, to the surrounding enamel, is likely to be sufficient to prevent bond failure.18 However, in such cases that the restoration is large enough to leave little surrounding tooth structure, successful orthodontic bonding is a challenge (Figure 2).
Figure 2.
(a) Amalgam bonding vs (b) banding on molar teeth.
Multiple studies have investigated different procedures for improved amalgam bonding.19,20,21,22 It is generally accepted that adequate bond strength can be achieved by a combination of:
Micromechanical retention via surface conditioning (diamond bur or sandblasting, as outlined above);
Chemical retention via a 4-META coupling agent.
4-META (4-methacryloxyethyl trimellitate anhydride) is an agent that increases adhesion to a number of surfaces, including metals. It contains two functional groups, a hydrophilic group and a hydrophobic group, both having an affinity for the metal oxides on the surface of amalgam and the composite resin used for bonding. This increases the surface energy of amalgam and so increases the wettability, thus leading to the ability to chemically bond to the resin.23
The combination of 4-META with surface conditioning has also been found to be suitable for bonding to other metal surfaces, including gold and stainless steel. However, in these instances, the bond strength is significantly weaker in comparison to amalgam18 and, therefore, orthodontic bonding to these materials remains a challenge.
Bonding to whitened teeth
Tooth whitening is an aesthetic procedure that is becoming more widely practised, as both in-clinic and at-home treatments. Dental bleach consists of either hydrogen peroxide or carbamide peroxide, along with stabilizing agents. Whitening is an oxidative bleaching process by which the peroxide molecules diffuse into the tooth surface and produce oxygen–free radicals and hydrogen peroxide anions.24 These molecules then travel through the enamel rods and into dentine, where they break down extrinsic and intrinsic coloured pigments, transforming them to colourless materials and therefore resulting in a lightened appearance.25
Following this process, the elimination of oxygen–free radicals from the enamel is not immediate and may remain for several days. Oxygen is an inhibitor of the composite polymerization process. Therefore, during this time, bonding with composite may be impaired due to the potential interference in the polymerization stage.24 Studies have also shown that the resin tags produced when etching bleached teeth, are smaller, more fragmented and penetrate to a shallower depth than in untreated enamel,26,27 again leading to a weakened bond strength.
Many studies have found the in vitro bond strength of composite to enamel is significantly reduced when placed within 24 hours of bleaching, however, a few studies in comparison have found the opposite.28In vitro studies have suggested the optimum time for bonding following bleaching to be 1−3 weeks, however, in vivo studies have given conflicting evidence, with no consistent suitable time frame.28 It is generally accepted that it is prudent to wait 7 days before composite bonding to whitened teeth and this is something that should be considered when planning orthodontic treatment.
With regards to traditional acid-etch technique vs self-etching primers, studies have shown that traditional etch and rinse systems give a higher bond strength than the self-etch systems.29,30 A postulated reason for this is that the hydrogen-peroxide agents may significantly decrease the enamel calcium and phosphate content.28 As previously discussed, self-etch primers work by dissolving the calcium from hydroxyapatite crystals, therefore bleached enamel with decreased calcium content will cause the self-etch primer to be less effective.
Bonding to enamel defects
Orthodontic bonding to a compromised enamel surface continues to pose a clinical challenge. Dental fluorosis is a developmental defect caused by increased exposure to fluoride during dental development. Fluorosed enamel has an outer hypermineralized and acid-resistant layer, followed by hypomineralized defects in the subsurface layer.31 These defects can present as discoloration (white or brown), pitting or striations. Studies using scanning electron microscopes have found that the hypermineralized enamel layer is unable to be effectively etched with 37% phosphoric acid, leading to irregularities in the etching pattern and therefore a decreased bond strength.32,33,34
There is paucity of evidence to identify the optimum bonding technique for enamel exhibiting moderate-severe fluorosis. Microabrasion with acid etch has been trialled and found to be effective, however, this is associated with poorer compliance with patients (due to the microabrasion process), increased chair-time, increased costs and irreversible damage to the enamel surface.34,35
Multiple studies have discussed the fact that the severity of fluorosis differs not only from tooth-to-tooth, but also from site-to-site on a single tooth surface.36 Due to this, it is difficult to conduct a reliable study and recommend a reliable treatment modality. Each case should be assessed on its own merit, but it is generally accepted that increased etching time will penetrate the hypermineralized enamel layer and potentially elicit higher bond strengths.
Amelogenesis imperfecta (AI) is a developmental abnormality of tooth enamel, resulting in poor development or complete absence of enamel due to the improper differentiation of ameloblasts.37 AI can affect both the primary and permanent dentition and has been shown to have a variable prevalence of approximately 1:4,000 to 1:14,000 in Western populations38 (Figure 3).
Figure 3.
(a) Severe AI with widespread enamel hypoplasia. (b) Mild AI with generalized mild pitting of the tooth surface. In these cases, it is important to remember that the altered tooth surface can cause differential expression of the prescription in the orthodontic bracket, due to the bracket base not sitting uniformly against the tooth surface. Therefore, it may be prudent to consider pre-orthodontic composite veneers on the worst affected teeth. This will serve to improve aesthetics for the patient and also allow more controlled expression of the prescription.
When treatment planning AI patients, it is important to complete a thorough examination of the weakened enamel surface. It is essential that the delicate enamel is deemed suitable to withstand not only orthodontic forces, but also the debond procedure. Conventional fixed appliance therapy can be used, but bond strengths have been shown to be less reliable.39 This can lead to multiple bracket failures, increasing treatment time and ‘burning out’ the compliance of patients who are likely to have already undergone extensive dental treatment. In order to overcome this, the use of resin-modified glass ionomer cement has been suggested. This adhesive system is less reliant on resin tag formation and will potentially also reduce further demineralization of the enamel surface, due to its fluoride properties.39 The use of ceramic brackets has been recommended for AI cases, as they are able to be removed with a high-speed handpiece. This avoids the use of traditional debonding pliers, which exert a high force on the tooth, and thus helps to preserve the delicate enamel surface. However, again, each case needs to be fully assessed and the method most suitable for the patient should be discussed with all involved.
Conclusion
Overall, the bonding of orthodontic brackets to atypical tooth surfaces poses a significant challenge to the clinician. Multiple methods for varying tooth surfaces have been described, each with their own merits and downfalls. Careful examination of the dentition is essential in order to allow the clinician to ascertain the best process for optimizing bonding to each individual tooth.
As part of the consent process, each patient should be specifically informed if he/she has a tooth structure that may lead to repeated bond failure, as this could significantly increase the treatment time. Multidisciplinary work with Restorative Dentistry colleagues can facilitate treatment for patients with dentitions that are already restored or will need further restoration. Use of indirect composite provisional crowns, for instance, can allow the placement of brackets more reliably in patients with significantly compromised tooth surfaces.
With the changing population undergoing orthodontic treatment, it is important that the specialty recognizes the associated difficulties in bonding and is aware of the techniques available to ensure that all patients are receiving the best possible care.