Carrotte P. Endodontics: Part 4 Morphology of the root canal system. Br Dent J. 2004; 197:379-383
Andreasen JO, Paulsen HU, Yu Z, Bayer T, Schwartz O. A long-term study of 370 autotransplanted premolars. Part II. Tooth survival and pulp healing subsequent to transplantation. Eur J Orthod. 1990; 12:14-24
Almpani K, Papageorgiou SN, Papadopoulos MA. Autotransplantation of teeth in humans: a systematic review and meta-analysis. Clin Oral Investig. 2015; 19:1157-1179
Snow SR. Esthetic smile analysis of maxillary anterior tooth width: the golden percentage. J Esthet Dent. 1999; 11:177-184
Tsukiboshi M. Autotransplantation of teeth: requirements for predictable success. Dent Traumatol. 2002; 18:157-180
Clokie CM, Yau DM, Chano LM. Autogenous tooth transplantation: an alternative to dental implant placement?. J Can Dent Assoc. 2001; 67:92-96
Day PF, Lewis BR, Spencer RJ, Barber SK, Duggal MS. The design and development of surgical templates for premolar transplants in adolescents. Int Endod J. 2012; 45:1042-1052
Shahbazian M, Jacobs R, Wyatt J, Willems G, Pattijn V, Dhoore E, Vinckier F. Accuracy and surgical feasibility of a CBCT-based stereolithographic surgical guide aiding autotransplantation of teeth: in vitro validation. J Oral Rehabil. 2010; 37:854-859
Day PF, Gregg TA.: UK BSPD National Clinical Guidelines in Paediatric Dentistry; 2012
Andersson L, Andreasen JO, Day P, Heithersay G, Trope M, Diangellis AJ International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 2. Avulsion of permanent teeth. Dent Traumatol. 2012; 28:88-96
The practical aspects of pre-operative assessment and surgical procedure for autotransplantation are discussed in this part of the series. The success of tooth transplantation is dependent on case selection, careful planning and a surgical procedure that maintains viable periodontal ligament cells and intact cementum of the transplanted teeth. A thorough assessment of the donor tooth and recipient site is vital for successful planning and execution of tooth autotransplantation. The surgical procedure involves atraumatic extraction of the donor tooth, socket preparation and splinting of the transplanted tooth. Post-surgical procedures include monitoring of pulp and periodontal healing and restorative camouflage of the donor tooth.
CPD/Clinical Relevance: Surgical planning and procedures are vital to the success of autotransplantation. Orthodontists should be aware of these factors and bear them in mind when preparing patients for autotransplantation to optimize surgical success.
Article
Surgical planning and technique are vital aspects to the success of autotransplantation. A number of key factors relating to the donor tooth and recipient site are considered during assessment and planning for autotransplantation.
Donor tooth assessment
Crown assessment
Donor tooth assessment is usually considered in terms of assessment of the crown and roots. A donor tooth crown should be assessed for dental caries, crown anomalies and crown dimension. One of the main considerations, when assessing the recipient site, is whether adequate space exists for the donor tooth. It is therefore essential that the donor tooth size is measured accurately at maximum bulbosity including the maximum bulbosity and cervical dimension of the crown. The mesio-distal widths of upper and lower premolars are usually only 1.5 mm smaller than that of upper central incisors (7 mm compared to 8.5 mm at maximum bulbosity), although the cervical areas are usually considerably smaller. To manage this discrepancy it has been suggested that rotating the donor premolar tooth approximately 90 degrees improves the emergence profile when transplanted into the upper central incisor region (Figure 1).
Figure 1. Placement of a premolar transplant into the socket of a maxillary central incisor postion demonstrating: (a) the difference in the mesio-distal crown widths at maximum bulbosity and the emergence profile at the cervical level between the premolar donor tooth and the contralateral central incisor; (b) the effect of rotating the donor premolar tooth to improve the mesio-distal crown width and emergence profile.
Root assessment
Donor tooth roots are assessed with regards to number of roots, stage of formation, morphology and dimensions in order to inform recipient site preparation. Single-rooted donor teeth with a single root canal system, such as mandibular second premolars, canines and incisors, are commonly the preferred choice due to their single root morphology and high frequency of single canal (85%) and single foramen (97.5%). The mandibular first premolars similarly have a single root morphology but the frequency of a single canal is lower (73%) and the likelihood of a single canal dividing into two apical foramens is higher (25%) than the mandibular second premolar. Maxillary second premolars are less commonly used as only 40% of cases demonstrate a single root with single root morphology canal system.1
Immature teeth are associated with better long-term success than mature teeth and present fewer restrictions in terms of bone height and tooth positioning. The ideal time for transplantation is when root formation is approximately 75% with an apical opening of at least 1 mm to encourage revascularization of the root canal bundle.2 In these teeth, the risk of transplant failure and subsequent extraction was reported to be 70% less than those teeth with closed apices.3
For teeth with complete root formation, careful selection is required as the root length can introduce height restrictions for positioning the donor tooth within the recipient bone. The average root length of premolars and canines is 13–16 mm. Such average root lengths provide an indication of the bone height required at the recipient site.
Radiographic assessment
Two-dimensional radiographs, such as long-cone periapicals and orthopantograms (OPTs), are usually sufficient for assessing donor tooth morphology and stage of root development (Figure 2). The use of cone-beam computed tomography (CBCT) is gaining popularity for pre-surgical assessment and can aid planning for potential donor teeth with unclear root morphology.
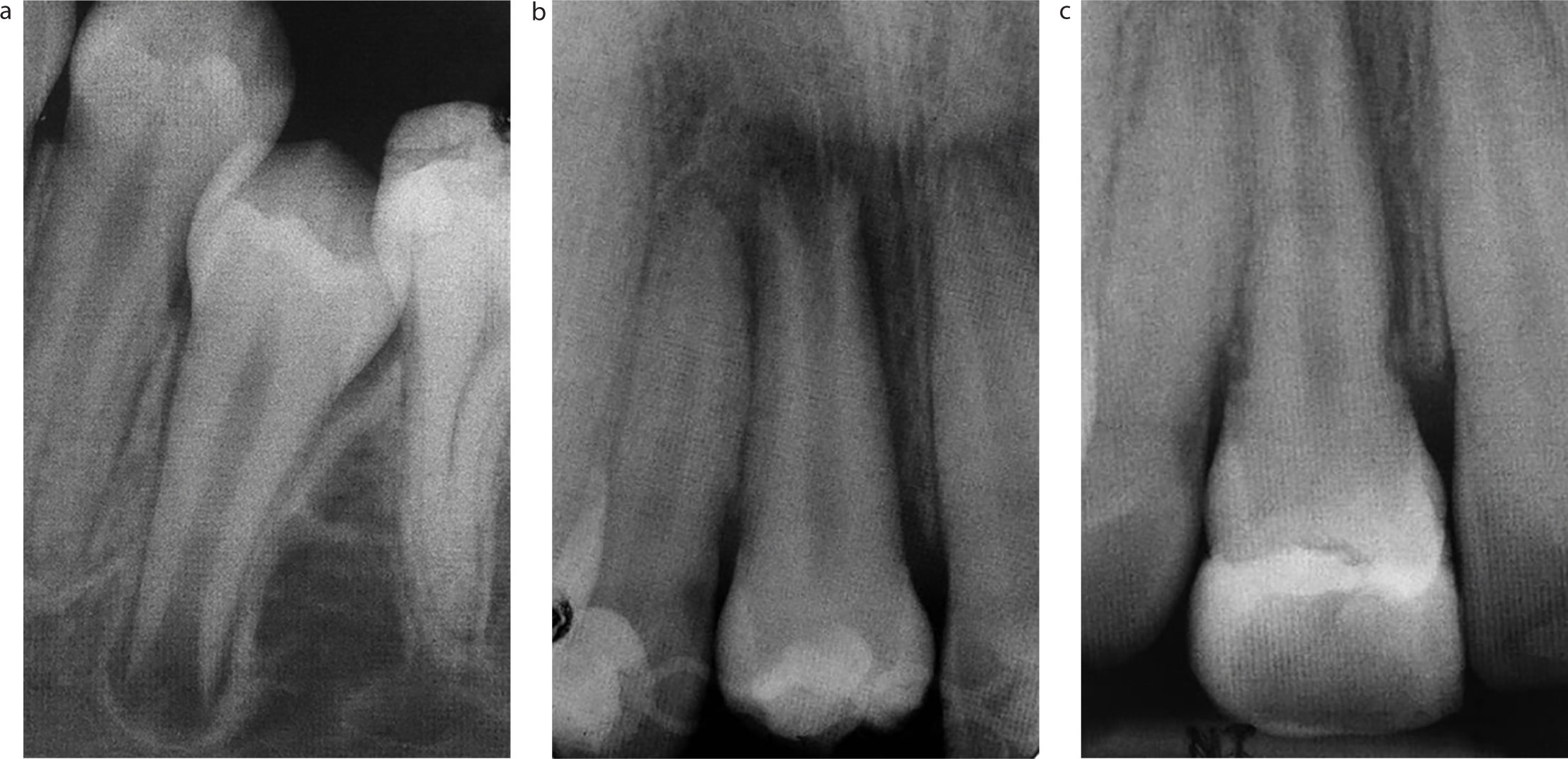
Figure 2. Radiographic examination showing: (a) potential donor tooth for transplantation to replace a maxillary central incisor. The second premolar was partially erupted with a single root and canal with incomplete root formation; (b) the transplanted premolar in the maxillary right central incisor position immediately post-operatively; (c) continued root development 6 months post-operatively.
Recipient site assessment
Clinical assessment
The recipient site should be carefully examined to assess bone volume, soft tissue morphology and the proximity of adjacent structures. Bone volume is assessed clinically by palpation of the alveolar ridge in order to identify bony deficits and soft tissue morphology, supplemented with appropriate radiographs (Figure 3). In a growing child, the alveolar bone is vulnerable to atrophy following tooth loss. To avoid alveolar bone loss in the recipient site, attempts should be made to maintain teeth in the recipient site, even if the prognosis of the tooth is poor. Teeth remaining in the recipient site should be monitored regularly for infraocclusion, which may cause a localized obstruction to vertical bone growth in the region leading to severe bony defects.
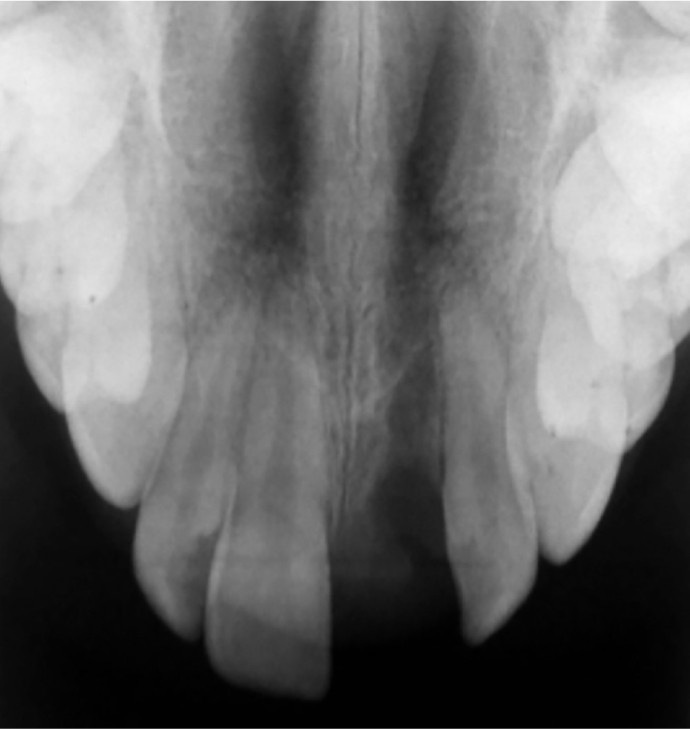
Figure 3. Upper standard occlusal radiograph used to assess bone levels in the maxillary left central incisor recipient site.
Coronal space is required between the teeth adjacent to the recipient site to enable placement of the donor tooth. Space requirements can be estimated by measuring the crown of the donor tooth. The space available in the recipient site should be measured at the gingival and incisal level. If the donor tooth is to be restored prior to definitive orthodontic treatment, sufficient space is also required for the restorative camouflage. In cases with single tooth transplantation, this can be estimated by measuring the contralateral tooth. In cases where a contralateral tooth is not available, the ideal coronal dimensions can be estimated from adjacent teeth using average relative proportions.4
The occlusion should be checked in static and dynamic function prior to or during surgery. This ensures that there is sufficient occlusal clearance to allow the transplant to be placed with minimal occlusal interferences. The transplant can be protected by the use of a removable appliance with posterior buccal capping if it is not possible to remove occlusal interferences prior to or during surgery.
Radiographic assessment
Radiographic assessment is crucial for assessing bone volume, the health of the teeth at the recipient site and proximity of adjacent structures. This assessment usually involves conventional radiographs (Figures 2 and 3) supplemented with 3-dimensional imaging, where further details are required. Radicular infection, infection-related resorption and any other pathology at the recipient site must be diagnosed and appropriately managed in order to optimize bone quality. The proximity of adjacent structures, such as adjacent tooth roots, the maxillary sinus and mental nerve, will impact on treatment planning.
Preparation for surgery
Preparation for surgery may be considered in terms of management of bone in the recipient site, space maintenance or creation and management of any pathology associated with failing teeth in the recipient site. Management of young patients prior to their entry into the autotransplantation care pathway should aim to maintain bone height and width. This may be difficult in cases where tooth loss was unavoidable, such as avulsed teeth that were not suitable for replantation, forced tooth extraction following complex injuries or persistent periapical pathology. Methods for managing the bone are described further in the fourth article in this series.
Teeth provide an ideal natural space maintainer and even teeth with poor long-term prognosis may be retained prior to autotransplantation to maintain space. In sites where the tooth has been lost, space should be maintained using a fixed or removable space maintainer, such as a temporary resin-bonded bridge or an upper removable appliance. In cases where space has been lost, pre-surgical orthodontics will be required to recreate the space, as described in the previous article.
Pathology in the recipient site should be managed in order to ensure optimal bone health at the time of transplantation. Pre-existing infection can be managed through disinfection of the root canal system, use of antibiotics, extraction of the tooth or surgical removal of the existing pathology.
Surgical technique
The choice for undertaking the surgical procedures using local analgesia, sedation or general anaesthesia will depend on the patient's age, co-operation, preference, medical history and the expected complexity of the surgery. Careful discussion with patients and those with parental responsibilities outlining the components of the surgical procedure and the advantages and disadvantages of each treatment modality is required for informed consent.
The surgical technique can be divided into five stages:
Extraction and assessment of the donor tooth;
Socket preparation;
Socket assessment;
Placement of the transplant;
Transplant splinting.
1. Extraction of the donor tooth
Extraction of the donor teeth using only coronal force application is performed to ensure minimal trauma to the root, and prevent damage to the periodontal ligament and cementum. Traumatic extraction with significant damage to the periodontal ligament is less likely to recover and will result in the transplanted tooth becoming ankylosed. In cases where there is more than one tooth available for transplantation, donor tooth selection is made based on root morphology, stage of development and anticipated ease of extraction. Direct visual assessment can be used to determine the root shape following extraction. The preferred donor tooth is then repositioned back into its original socket to prevent damage to periodontal ligament cells while the socket is prepared in the recipient site.
2. Socket preparation
The steps required for socket preparation depend on the presence or absence of a tooth in the recipient site. Preparation of existing sockets is easier than creation of new ones in an edentulous alveolar ridge. Socket preparation for a recipient site with a poor prognosis tooth is shown in Figure 4.
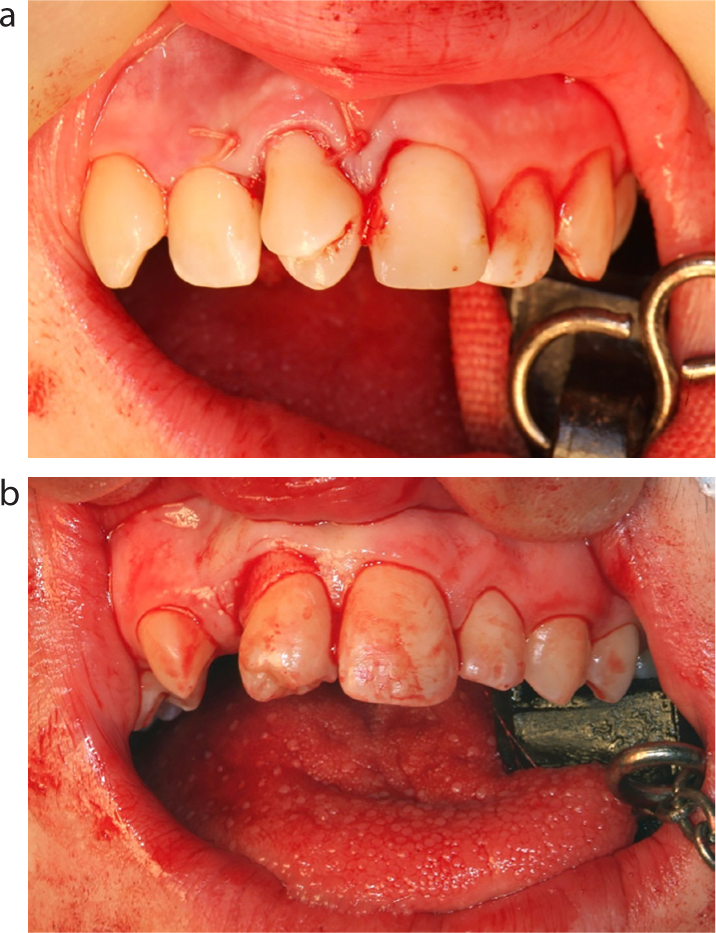
Figure 4. Surgical steps involved in transplantation of the mandibular second premolar (LL5) into the maxillary right central incisor (UR1) position: (a) infra-occluded UR1 judged to have poor prognosis due to replacement resorption following avulsion and replantation; (b) extraction of the UR1 at the time of the transplantation; (c) atraumatic extraction of the LL5; (d) the use of a surgical template to assess the depth and width of the donor site socket; (e, f) the use of a surgical bur (e) and osteotomes (f) to modify socket depth and width; (g, h) transplantation of the donor tooth into the prepared socket and confirmation that there are no occlusal interferences on the transplanted tooth; (i) the transplant is splinted using a titanium trauma splint.
3. Socket assessment
The socket is assessed during preparation to ensure that it is able to accommodate the donor tooth. Traditionally, this was achieved by transplantation of the donor tooth into the prepared socket. Several attempts are usually made before a suitable socket is created, which risks further damage to the periodontal ligament cells and increases the risk of future ankyloses.5 Consequently, different techniques have been proposed to aid assessment of socket height and width (Figure 5). These include pre-surgical radiographic measurements,2 acrylic stents constructed using radiographic measurements,6 surgical metal stents constructed using average measurements of premolar teeth7 and construction of 3D tooth replicas using Cone-Beam Computerized Tomography (CBCT).8 Pre-fabricated surgical templates assist the surgical component of premolar transplantation by establishing and replicating the root dimensions of the donor premolar tooth. The correct template is used to assess the width and depth of the socket preparation prior to placement of the transplant in the recipient site.
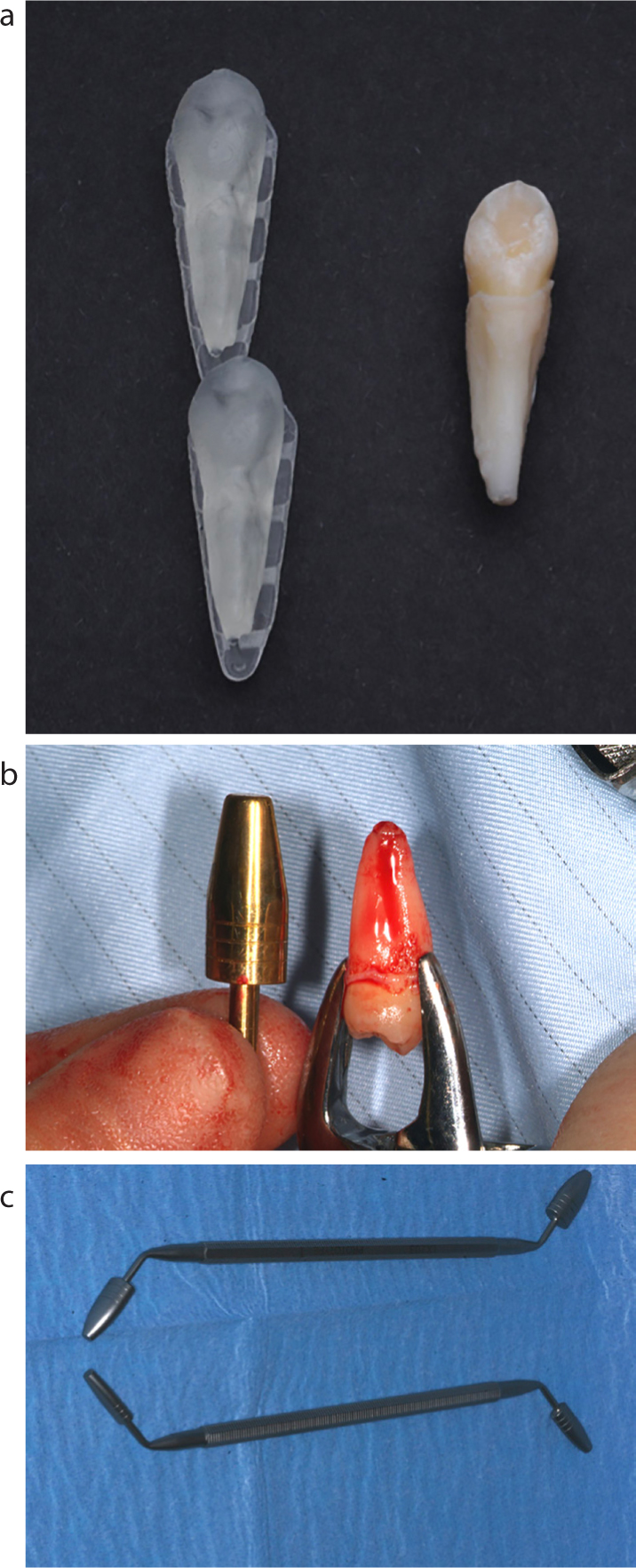
Figure 5. Different methods of replicating the transplant tooth to aid surgical preparation of the socket for the transplant: (a) 3D printed stents developed from a cone beam scan of the donor tooth; (b, c) two different designs of pre-fabricated surgical templates. The correct size can be selected based on the proportions of the donor tooth.
4. Placement of the transplant
The transplanted tooth should ideally be seated a few millimetres from the occlusal plane to prevent occlusal trauma and damage to the periodontal ligaments. This has the additional advantage of allowing the tooth to erupt into a functional position with corresponding bone deposition. Transplants with complete root formation require root canal treatment, therefore coronal reduction could be performed at time of transplantation, if required. On the contrary, particular care should be taken with immature teeth, as revascularization is desirable and may be compromised by enamel reduction. If ideal positioning is not possible, occlusal reduction of immature teeth could be undertaken gradually to optimize pulp recovery. Positioning immature teeth in relation to the occlusal plane is less critical as these teeth have the potential to erupt, encouraging bone growth and improved gingival contour.
5. Transplant splinting
The transplanted tooth is splinted using a physiologic splint such as a titanium trauma splint (TTS) with the transplanted tooth splinted to at least one tooth on either side (Figure 4g). Sutures are reported for splinting teeth, particularly where no adjacent teeth are available for bonding a splint, but care must be taken to ensure that the sutures provide adequate stabilization of the transplanted tooth. The splint should be passive to prevent damage to periodontal cells and attached to the teeth with composite.
Antibiotic prophylaxis
There is little evidence for use of systemic antibiotic administration after transplantation. Although a positive effect has been demonstrated in several studies for prophylactic systemic antibiotics with avulsed and re-implanted teeth, there is limited evidence to support their use in autotransplantation where the conditions are controlled.9,10 A recent systematic review and meta-analysis has shown that the failure rate and occurrence of infection-related resorption of tooth autotransplantation were 2.5 times and 1.4 times higher in studies where no systemic antibiotics have been used, respectively. Therefore, the use of systemic antibiotics, albeit controversial, seems to be beneficial in tooth autotransplantation.
Short-term post-surgical care
Post-operative instructions
Post-surgical instructions for autotransplant patients are given as follows:
Appropriate analgesia to manage any post-operative pain;
Meticulous oral hygiene to encourage healing and prevent infections;
Use of a Chlorhexidine Digluconate mouthwash (0.2%) or gel (1%) to support oral hygiene, particularly during the first few days post-operatively while brushing may be difficult;
A soft diet is recommended for two weeks following the procedure to prevent detachment of the splint and movement of the transplant;
Contact sports are prohibited during the recovery period.
Pulp and PDL management
Patients are reviewed, following the autotransplantation, after 7–10 days to assess recovery and healing. Clinical examination focuses on:
Oral hygiene assessment and reinforcement;
Periodontal healing of transplanted tooth;
Pulp extirpation for teeth transplanted with complete root formation;
Splint removal with assessment of transplant mobility and gingival healing;
Mobile transplants or those with inflamed gingival tissues should be splinted for a further week;
Interim restorative camouflage of the transplant (Figure 6).
Figure 6.
(a, b) Interim restoration placed on the transplanted premolar in the maxillary right central incisor position for the duration of orthodontic treatment.
Interim restorative camouflage
At the review appointment, an interim temporary restoration can be provided to improve the appearance of the transplant if required. This has the advantage of improving aesthetics and normalizing the coronal morphology for positioning adjacent teeth; however, it may also obscure the transplant morphology during orthodontic tooth positioning and increase plaque stagnation. Firm transplants with healthy gingiva can be camouflaged using direct composite veneers.
Medium term care
Monitoring healing
Transplanted teeth are then followed up clinically and radiographically following the same guidelines for avulsed and replanted teeth. The initial follow-up appointment is after 7–10 days where splint removal and the interim composite camouflage restoration is placed. For transplants with closed apices, where revascularization is not expected, pulp extirpation is performed at this appointment. This is followed by an appointment 4 weeks post-transplantation for completion of endodontic treatment with definitive obturation. The transplant is then reviewed clinically and radiographically at 3 months, 6 months and 12 months.
Transplants are assessed in relation to:
Oral hygiene and gingival health;
Clinical signs and symptoms of periapical pathology (pain, tenderness to percussion, mobility and sensibility testing in immature teeth);
Clinical signs of ankylosis (infraocclusion, altered percussion sound);
Radiographic signs of replacement resorption, pathology and root resorption.
Definitive restoration
Following completion of orthodontic treatment, a definitive restoration can be provided if required. Composite veneers are preferable to porcelain veneers as modification to address continued growth and gingival maturation is easier. Adjunctive treatments, such as gingival re-contouring and tooth bleaching, can be used to improve the aesthetic outcome (Figure 7).
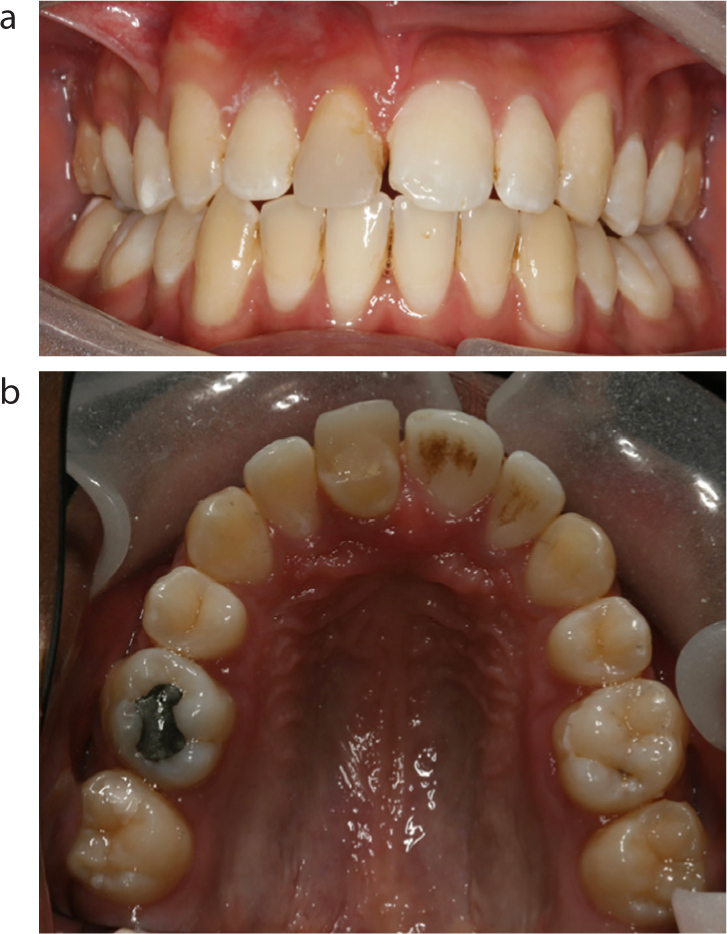
Figure 7.
(a, b) A transplanted premolar replacing the maxillary right central incisor (shown in Figure 6) following definitive restoration. This involved single tooth bleaching of the premolar transplant followed by placement of a porcelain veneer.
Conclusions
Successful autotransplantation relies on careful pre-surgical assessment of the donor tooth and recipient site. The recipient site is prepared to optimize the bone quality and health. Surgery aims to remove the donor tooth atraumatically, preserving the periodontal ligament. The transplant is placed into the prepared recipient site and splinted during the healing period. A standardized review protocol is followed to ensure that transplant healing is monitored and timely follow-up orthodontic and restorative care is provided.