The best of both worlds? combining specialist practice with hospital consultancy Dental Update 2024 12:2, 707-709.
Abstract
This article describes the experience of undertaking post specialty consultant training, on a part-time basis, with its advantages and disadvantages, and how this experience is transferred into a current practice combining a hospital consultant and specialist practice position, with its challenges and benefits.
CPD/Clinical Relevance: The workforce providing primary and secondary care orthodontics is evolving and it is important that alternative training modalities and working practices are available to allow flexibility in provision of care.
Article
In an ever changing world there appears to be uncertainty in everything around us and this is no different in the world of dentistry and the specialism of orthodontics. NHS funding for both primary and secondary care orthodontics is under pressure1 and, in a specialty which was previously primarily based on adolescent patients, a new, ever increasing private adult market has evolved.2
This had led to a change in the make-up of the workforce with a blurring of the lines between primary and secondary care providers, with many orthodontists trained to NHS consultant level spending part of their week in primary care.3
This article is in two parts, part one describes one of the author's experience undertaking his Post CCST consultant training, on a part-time basis, with the advantages and disadvantages, part two of the article illustrates the two authors' current working weeks combining hospital consultant positions and specialist practice positions, with its challenges and benefits.
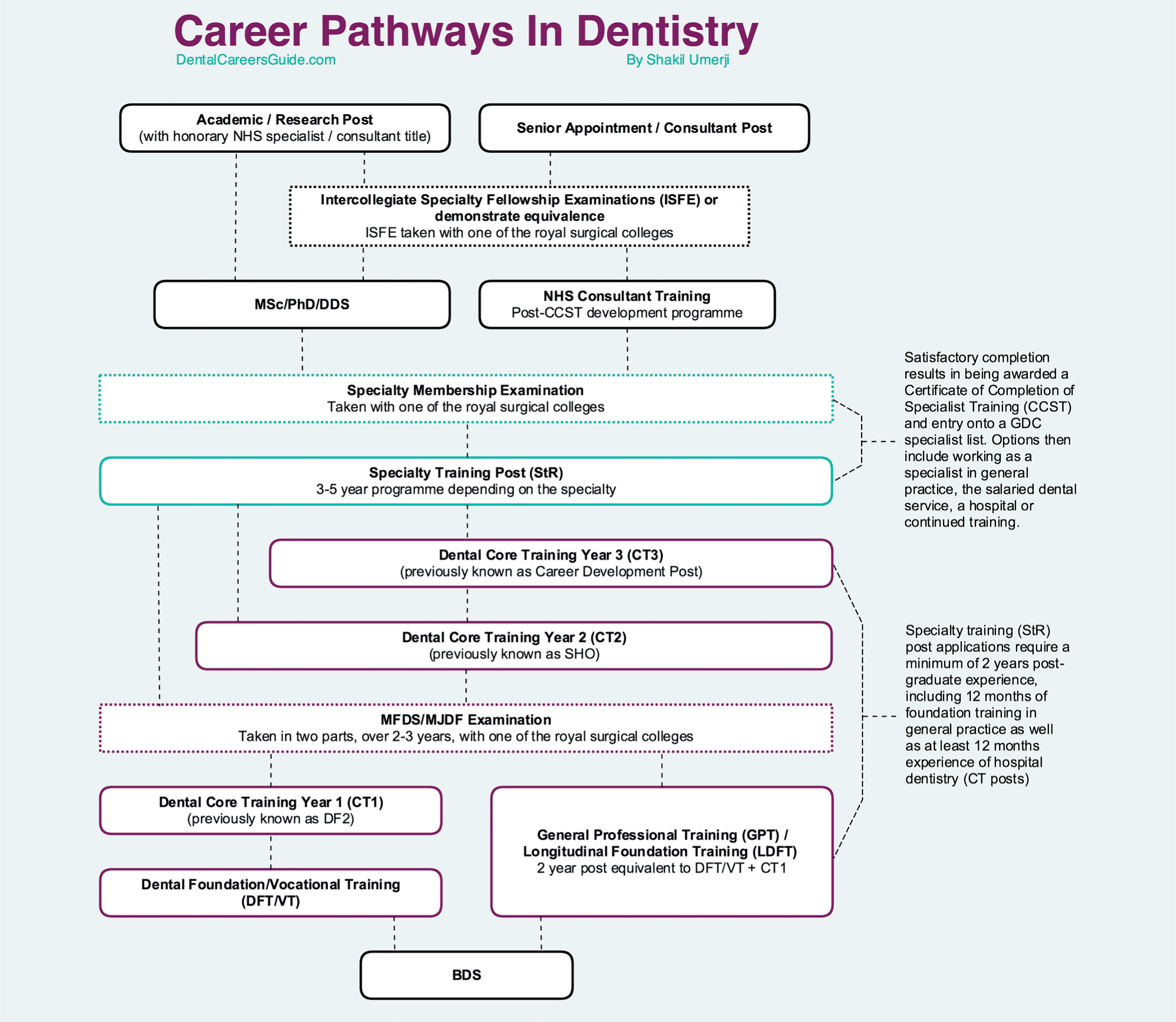
In the United Kingdom, orthodontic training is currently structured in the following way. A three year specialist training programme4 incorporating a higher research degree based between a University Teaching hospital and District General hospital, which is accessed by competitive entry through national recruitment, with limited training numbers available per year, which are funded through the deaneries by NHS England.
Successful completion of training4 (CCST), a research degree undertaken during the training period and successful completion of the Membership in Orthodontics (MOrth) examination from one of the royal colleges allow access to the General Dental Council's specialist register in orthodontics. The trainee would then be able to work in primary care specialist orthodontic practice and use the title Specialist in Orthodontics.
Following successful completion of specialist training, an option of a further two years of training can be undertaken5 (Post-CCST), which is accessed by competitive entry and is funded by NHS England, which allows the trainee to sit the intercollegiate specialist fellowship exam (ISFE). If successful, this enables the orthodontist to apply for secondary care consultant orthodontist positions within the NHS and use the title Consultant in Orthodontics. There are also some ‘run through’ training posts where the trainee can continue past 3 years, if MOrth is gained, and go on to complete the ISFE in the next 2 years. The career pathways in dentistry is illustrated in Figure 1.
Figure 1. Career Pathways in Dentistry. DentalCareersGuide.com
Consultant positions within NHS hospitals are usually involved in the treatment of patients with more complex malocclusions, requiring multidisciplinary treatments, combined orthognathic surgery and cleft-related treatment.
Part 1: Part-time training My training experience by Paul Scott
I completed my specialist registrar orthodontic training in September 2007 and I was undecided between undertaking a fixed term training appointment (FTTA) or consultant training (Post CCST training) and entering specialist orthodontic practice, as I suspect a great number of people are at this stage.
Both routes had different appeals but family circumstances dictated a relocation to Leeds and I entered full-time specialist orthodontic practice, in Leeds, in the October of 2007. I spent the next two years exclusively in specialist practice developing my orthodontic diagnostic and clinical skills, but my desire to undertake the additional training had not subsided and, when a FTTA post was advertised in the summer of 2009, in the Yorkshire region, I approached the deanery regarding the possibility of undertaking training on a part-time basis.
My initial contact was to the then Postgraduate Dean for Dentistry (Mr Paul Cook) for the Yorkshire and Humber region. He actively encouraged my application for the post on a part-time basis and he outlined how part-time FTTA training could be structured, and the difference compared with people undertaking less than full-time training posts. (Part-time training as the name suggests is training undertaken on a part-time basis from the outset, with the clinician only contracted for the number of sessions specified with the training time adjusted accordingly, but with the freedom to work on the non-contracted sessions. Less than full-time training6 (LTFTT), previously known as flexible training, is usually undertaken for personal/childcare reasons and is often implemented during the training period, with the training time extended, but excludes the trainee from undertaking any additional work – see the Dental Gold Guide6). My next contact was with one of the regional consultants who was also very positive and once again outlined how it could work in the region; he also made it clear that it would not be easy combining a training post with all the additional responsibilities and duties, whilst working half the week in a busy orthodontic practice, but he noted that, as long as I was flexible and had good time management, it was a viable option.
Following a successful interview, I found myself, in combination with the second author, starting FTTA training on a part-time basis, to be undertaken on a 50% basis over 4 years. My rotation was the Leeds Dental Institute and York District hospital, to be undertaken on a 5 session basis, with time-tabled clinics all day Monday and Friday, with an administration session timetable for Thursday afternoon that essentially was floating, allowing flexibility in the timetable. In preparation for my new part-time hospital role, I made a number of alterations to my working week in specialist practice. This included employing a clinical assistant to help with some of the more basic workload and extending one of the evening sessions to provide more flexibility for the patients.
Initially I found it difficult to adapt between the roles of hospital and specialist practice, with frustration especially within the dental hospital at the perceived inefficiency in the patient journey in comparison to specialist practice. One of my consultant trainers helped to reduce this frustration by explaining that the dental hospital service had a number of limiting factors, mostly due to its training role and complexity of patients, and could not be compared to my sessions in specialist practice for efficiency. I also found that my extra curricula duties at the start outweighed my dedicated administration session time, with multidisciplinary clinics to prepare, projects to undertake, journal club presentations, research and teaching commitments. As in any job, things settled down once I had found my feet and I had prioritized my jobs and adjusted my week to allow more time at home to undertake hospital-related work. At this stage, I started to plan how the next four years would be structured with regards to filling the commitments required for FTTA training in relation to receiving the appropriate training and gaining the correct experience, undertaking the correct number of complex cases, completing audits, undertaking research and planning at what stage to undertake the Intercollegiate Specialty Fellowship Examination (ISFE).
My plan was as follows:
Year 1: to use year one to find my feet and collect the correct mix of complex patients required for my training, along with taking a major role in developing a protocol and gaining ethical approval for a regional randomized controlled trial (RCT) into the effectiveness of two forms of orthodontic retention, that would be used as a research project for two of the next intake of first year StRs entering the orthodontic training programmes in Leeds.
Year 2: this was to increase the number of joint clinics being attended, undertake a large scale audit in York, increase my teaching skills and develop a number of projects I had been given.
Year 3: this would be used to refine my clinical skills, knowledge and prepare to sit the ISFE at the end of year three (18 months pro-rata, which at the time was the minimum requirement).
Year 4: to use year four to complete existing patients, finish any outstanding projects and target clinical learning to areas of weakness.
I used this plan as the outline for my personal development portfolio (pdp) and presented it at my first RITA (Record of in Training Assessment) at the end of year one. The RITA was the forerunner of the Annual Review of Competence Progression (ARCP), which provides a formal process that uses the evidence gathered by the trainee, relating to his/her progress in the training programme. It should normally be undertaken on at least an annual basis for all trainees undertaking specialty training and will enable the trainee, the Postgraduate Dean and employers to document that the competences required are being gained at an appropriate rate and through appropriate experience. The process may be conducted more frequently if there is a need to deal with performance and progression issues outside the annual review. It is not in itself a means or tool of assessment.
My part-time FTTA post was completed at the end of September 2013 and I followed my pdp as set out in Year 1. The whole experience was superb and I think as a training modality it lends itself perfectly to FTTA (post CCST) training.
There are a huge number of benefits for undertaking the training over an extended period that include:
The ability to start and complete a large number of cases which, from a training perspective is excellent. This allows you to be able to take your orthognathic patients through the full process from start to finish. Alveolar bone graft patients can be followed up and the hypodontia patients can be debonded, have their definitive restorations placed and monitored in retention. One of the major benefits of this is that I did not have to take on many transfer patients as I would see all stages of patient care throughout my training period.
The extended period of training allows for better workforce planning in the training units as the cohort of patients taken on for treatment by the part-time trainee should have completed treatment by the time he/she leaves, allowing the job plan/clinic template to be amended in the final year, if number of patients in treatment decreases to allow the trainee to undertake more new patients clinics, undergraduate teaching, etc.
The ability to work in specialist practice means that a large number of cases are undertaken and a range of appliances can be used; this definitely improves basic clinical and diagnostic orthodontic skills and this leaves the part-time trainee with a huge advantage over a full-time trainee, when both finish their posts. It also develops a definite skill in treatment/time efficiency due to the busy nature of specialist practice.
As the training period is over an extended period, this allows more access to multidisciplinary clinics as these can often be once per month. My timetable included two joint orthognathic clinics per month, one in each unit, and a joint restorative clinic once per month. I also had access to further Cleft, Paediatric dentistry, Restorative, Craniofacial and Distraction clinics on an ad hoc basis, depending upon training needs at the time and my availability.
The extended training time has also allowed me to undertake larger projects that would not be possible in a 2-year period.
Flexibility and the ability to prioritize has been extremely important whilst undertaking the training on a part-time basis, as there are often clinics, meetings, teaching sessions and courses that are not in your weekly hospital sessions. This needs good time management skills which are definitely developed with part-time training. There will be certain sessions that you need to attend for your own training and things that can be put off for another time and obviously this needs the flexibility in your specialist practice sessions to be able to rearrange which days you are working, to ensure that neither the hospital nor specialist practice sessions suffer.
As I have discussed the benefits of part-time training, I should discuss the disadvantages, of which I find it difficult to find many. One disadvantage could be seen as only being in each unit once per week and, with required training courses and holidays, you may not be able to attend a unit for a number of weeks at a time. This can lead to a feeling of detachment from the unit, but with email communication and the support of colleagues I didn't find this too much of a problem. There are other disadvantages, depending on the number of FTTAs in the region. When I started, there were only 3 FTTAs (1 full-time and two part-time) in the West Yorkshire region. Additional duties and jobs were shared between the three of us and, as a part-timer, I felt overloaded in comparison to the amount of sessions I worked. This did, however, teach valuable skills in being able to say no when offered jobs and explaining what I was already undertaking.
My feedback from the Deanery is that they have found the whole process beneficial with regards to the part-time training that Andrew and I have undertaken, with the sum of the two parts having delivered more than one whole time appointment.
Part 2: Part-time hospital consultancy/part-time specialist practice
Following the completion of Post-CCST training, the aim of both the authors was to develop a split working week, part-time as a hospital consultant and part-time in specialist practice.
Initially, Andrew undertook two separate locum consultant positions whilst continuing in specialist practice three days per week. I returned to full-time specialist practice whilst waiting for a suitable part-time consultant position. I also took the role of MCN Chairman for West Yorkshire at that time as, with experience in both primary and secondary care provision, I thought that I could be helpful in the negotiations of the future orthodontic commissioning.
Andrew's locum position at the Montagu Hospital in Mexborough, part of Doncaster and Bassetlaw NHS Trust (Figure 2), allowed him to assess the pros and cons of the unit without long-term commitment and, when it became apparent that a full-time senior consultant would be retiring in the near future, Andrew approached me and discussed the option of a potential job share for the position that would become vacant.
The Montagu Hospital in Mexborough already had a history of part-time orthodontic consultants with two part-time consultants and one full-time consultant. Hospital management were forward thinking and could already see the benefit of part-time working patterns and the flexibility that it brings to the department and hospital in general.
Andrew and I approached the existing consultants and the management team on their thoughts on our application for a job share of the upcoming post. Both the existing consultants and the hospital management were extremely supportive and actively encouraged us to apply for the post that would be available in six months. At that stage, I also undertook a locum position within the Trust to help with the potential transition into the unit, bearing in mind that a permanent position was dependent on a successful interview process. This provided continuity of care for the cleft lip and palate patients, as I would be taking over the cleft lead as part of my role. With the two of us working as locum consultants, this allowed us to develop two job plans that would be suitable for both me, Andrew and the existing clinical and management teams.
At that stage my working pattern within specialist practice required some alteration to fit around the hospital commitments. The late evening was moved to a Monday and the therapists and DWISIs' days were adjusted, with an additional session to be worked by one of the DWISIs so that the correct supervision was available for each group of clinicians. Extra fracture sessions were placed in the book for the days that I would be off site to provide a full week of cover for the specialist practice patients. Both authors were successful at interview for the eventual two part-time positions that were advertised and have now been in their consultant positions for a number of years and split their working week between hospital consultant positions and specialist orthodontic practice.
Tables 1 and 2 illustrate the split in the working weeks along with the roles the individuals undertake during the working week shown below.
Day
Monday
Tuesday
Wednesday
Thursday
Friday
Location
SpecialistPractice (extended hours until 7pm)
SpecialistPractice
SpecialistPractice
Hospital
Hospital/Specialist practice (alternate weeks)
Supervising Therapist/DWISI
Supervising Therapist/DWISI
Supervising Therapist/DWISI
Supervising Post-CCST/Therapist
Supervising Therapist/DWISI
Clinic Type
NHS/Private
NHS/Private
NHS/Private
Hospital Treatment ABG clinic
Multidisciplinary clinic Orthognathic/Cleft
Day
Monday
Tuesday
Wednesday
Thursday
Friday
Location
Specialist Practice
Hospital
Specialist Practice
Specialist Practice (extended hours until 7pm)
Hospital (alternate weeks)
SupervisingTherapist
Supervising Post-CCST/Therapist
SupervisingTherapist
SupervisingTherapist/DWISI
Clinic Type
NHS/Private
Hospital Treatment
NHS/Private
NHS/Private
MultidisciplinaryclinicOrthognathic
Paul Scott's current roles and working week (Table 1)
Consultant Orthodontist and Cleft Lead for Doncaster and Bassetlaw NHS Trust;
Specialist Orthodontist Orthosolutions, Leeds;
Specialist interests treatment of cleft lip and palate, orthognathic surgery, complex hypodontia, adult orthodontics, invisalign treatment;
Management commitments, teaching;
Educational supervisor role StR;
NHS contract provider, private practice, supervising orthodontic therapists and DWISI;
Chairman of the West Yorkshire orthodontic MCN;
Andrew Shelton's current roles and working week (Table 2):
Consultant Orthodontist Doncaster and Bassetlaw NHS Trust;
The advantages and disadvantages of a primary and secondary care working split are illustrated below:
Advantages:
Varied workload;
Financial benefits with a potential improved job security. In a changing landscape there could be a shift in emphasis from secondary to primary care;
Full range of appliances used, not limited by NHS constraints;
Teaching, management roles in the hospital;
Practice principal and business roles;
Cross pollination of techniques from each setting enhancing clinical skills.
Disadvantages:
Commitment clashes;
Not always having the ability to complete a task as the following working day could be in a different setting. In the digital age, however, it is often possible to complete tasks when off site.
It is worth pointing out that, having multiple part-time consultants in one department can be perceived to lead to issues with continuity of care/training, attendance at meetings and conflicts of opinion. Our experience is that, with a good team ethic and careful planning of clinics, our current department of four part-time consultants works extremely well. Flexibility of job plans has led to our development of a multidisciplinary orthognathic clinic that all four orthodontic and two oral and maxillofacial consultants attend. This allows for cross-checking of treatment plans, improvement in clinical governance and has not lead to a significant change in efficiency. Attendance at monthly clinical governance meetings can be an issue, but this has been overcome by rotating the meeting day each month and providing a teleconference service for off-site consultants. Overall, it is our opinion that, with careful planning and good teamwork, the advantages of multiple part-time consultants versus fewer full-time consultants outweigh the disadvantages for both the Trust and the individual.
We have often been asked what did you get from part-time training that benefits your current working practice, in comparison to individuals undertaking full-time training?
This is a very subjective question to answer but this article illustrates that, in the authors' eyes, the advantages of part-time post CCST training far outweigh full-time training. It must be remembered that the individual must be ready for the extra workload and sacrifices that have to be made, but the reward at the end of your training is that you have the potential to develop far more of your clinical time and management skills. The initial intention of both authors was to attempt to have a working week very similar to their current roles at the start of their FTTA training. The advantage to both of us was that we were effectively preparing ourselves for our future roles of part-time consultancy and part-time specialist practice. This meant that this transition was relatively straightforward and we could build on the skills that we had already learnt. Learning to cope with a split working week after full-time training is perfectly feasible and we both feel that a trainee can potentially come out of part-time training better equipped. One clear benefit from working in specialist practice during your training is that your clinical experience, speed and efficiency improve. In addition to this, you are definitely exposed to the financial side of delivering clinical treatment and this awareness means that cost/efficiency savings learnt from primary care can be implemented in secondary care. This is extremely important in the current NHS financial climate.7
Summary
This has been a great training experience and we consider ourselves very privileged to have undertaken FTTA training on a part-time basis and, if we were offered the same opportunity again, at the same stage, we would definitely take it. There are a huge number of positives to undertaking the training in this manner which outweigh the negatives. We do think that this is a beneficial way to undertake the additional training to consultant level and this can bring many advantages that can be taken into the working future. Although this article only represents the opinion of two clinicians who have been through the training, it does demonstrate that that there are definite benefits in offering part-time post-CCST training in the future.