Professor and Head, Department of Orthodontics and Dentofacial Orthopedics, Manipal College of Dental Sciences, Manipal University, Manipal — 576104, Karnataka, India
This case report demonstrates treatment of an open bite case with a history of trauma to the maxillary anterior region in childhood. A 20-year-old adult male presented with a convex profile and significant anterior bite and unilateral posterior crossbite. Surgical bite correction was planned but posed a dilemma in the choice of surgery.
CPD/Clinical Relevance: To demonstrate the outcome of a case of skeletal anterior open bite treated with orthognathic surgery.
Article
An anterior open bite is an inability of maxillary and mandibular anterior teeth to contact or overlap in a centric relation.1 Abnormal growth, trauma, heredity, habits or tongue position, septum problems, enlarged tonsils and adenoids are proposed aetiologies.2 Various treatment options include vertical pull head gears, posterior bite blocks, functional appliances, multi-loop edgewise appliance or orthognathic surgery, depending upon the age of the patient. Jaw imbalances and improper bites in growing age groups can be treated with head gear and functional appliances, while adult age groups are usually treated with orthognathic surgery to improve function and aesthetics.
Case report
A patient reported to the Department of Orthodontics with an inability to touch the front teeth. He reported a history of trauma to the maxillary anterior region in childhood, after which he noticed that the gap between the front teeth increased with age.
His extra-oral examination revealed a convex profile, increased lower facial height, a steep mandibular plane angle and thick procumbent lips. Smile analysis showed a maxillary arch canted to the left-hand side. Intra-oral examination showed a Class I molar bilaterally and crossbite with respect to the posterior right-hand side in the molar and premolar region. The patient also had a tongue-thrusting habit. The upper midline was deviated to the right-hand side by 2 mm. The lower central incisors LL1 and LR1 showed gingival recession of 2 mm and 1 mm, respectively.
Cephalometric records (Figure 1) and plaster models were prepared. Cephalometric analysis revealed a maxillary skeletal base tipped upwards. The final diagnosis for the patient was skeletal Class II and dental Angle's Class I malocclusion with the maxilla canted to the left-hand side and an upper midline deviation by 2 mm to the right-hand side with a tongue-thrusting habit.
Figure 1.
(a, b) Pre-treatment radiographs.
Treatment objectives
Correction of tongue-thrusting habit.
Co-ordination of upper and lower arches.
Correction of the Class II skeletal pattern.
Correction of the maxillary cant.
Correction of the unilateral posterior crossbite and improvement in bite.
Achievement of a Class I incisor relationship with an ideal overjet and overbite.
Periodontal treatment of lower gingival recession.
Treatment options
The patient was an adult, so growth modification procedures were out of the question. The only choice was between orthodontics alone and orthodontics plus surgical treatment.
Non-surgical treatment with fixed orthodontics and the use of posterior bite blocks and implants plus box elastics to close the bite.
Limitations: This would have led to over extrusion of upper incisors and smile line becoming unaesthetic. The mandibular plane would have improved mildly. The profile change would have been minimal.
Combined orthodontics and surgical treatment. The dilemma was in the choice of surgery.
Options were:
Lefort 1 osteotomy with an asymmetric posterior impaction to correct the cant;
Lefort 1 osteotomy with a Surgical-Assisted Rapid Palatal Expansion (SARPE);
Lefort 1 osteotomy combined with a bilateral sagittal split osteotomy (BSSO) to close the bite;
A bilateral sagittal split osteotomy (BSSO) to advance the mandible and close the bite;
An anterior maxillary subapical osteotomy to down position the maxillary anterior area.
Limitations: Option 2 would have split the maxilla into multiple pieces, option 5 would have increased incisal show at rest considerably. Option 4 would have closed the bite but the maxillary cant would have been unaltered. So, out of options 1 and 3, option 1 was chosen as it addressed most of the problems. Also, superior impaction shows the maximum stability among surgeries.
Treatment plan
Combined surgical orthodontic plan to correct the bite and malocclusion
Segmental alignment of the upper arch and continuous alignment of the lower arch;
Co-ordination of the upper and lower arches;
Surgery – asymmetric impaction of the maxilla with Lefort 1 osteotomy (option 1) and auto-rotation of the mandibular arch;
Post-surgical finishing and debonding.
Treatment progress
Pre-surgical procedure
Treatment started with the patient being educated about the tongue posture and interception of the tongue-thrusting habit with elastic swallow exercises. This was followed by the placement of 0.022″ pre-adjusted edgewise brackets and molar tubes (MBT Victory series, 3M, UNITEK, Monrovia, CA, USA).
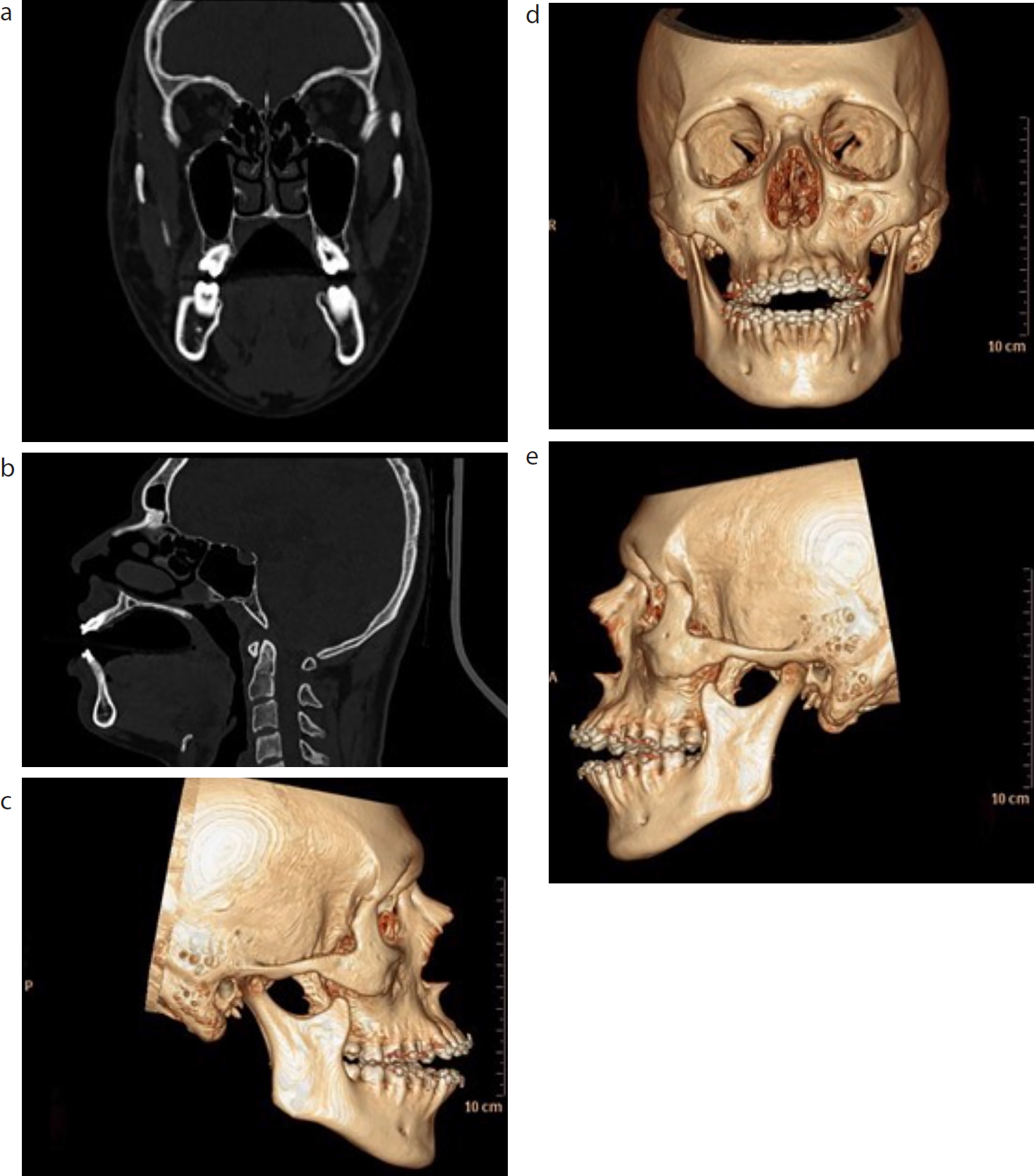
Levelling and alignment with 0.016″ NiTi archwire (d-tech, Wagholi, Pune, India) and well co-ordinated 0.018″ stainless steel (SS) archwires (AJ Wilcock Premium Plus Australian archwire, Whittlesea, Victoria, Australia) was carried out. However, sectional alignment was carried out in the maxillary canine to canine region and the posterior segments to avoid extrusion of the upper anteriors. 0.019″ × 0.025″ stainless steel wire (Truforce, Ortho Technology, Inc, Tampa, USA) was then placed with hooks to finish the pre-surgical phase (Figures 2 and 3). The patient was then referred to the Department of Oral Surgery. A pre-surgical CT scan was performed (Figure 4). After planning mock surgery on the patient's casts, a surgical splint was prepared.
Under aseptic conditions and general anaesthesia, local anaesthesia was given in the maxillary region. Markings were made for the osteotomy cut with a pencil. A Lefort 1 osteotomy was performed with asymmetric impaction of the maxilla. Since the maxilla was canted, impaction of 5 mm on the right-hand posterior and 3 mm on the left-hand posterior sides were carried out. The teeth were guided into the desired occlusion and maxillomandibular fixation was performed using 0.026″ gauge wire. Five plates were fixed with screws, after which the inter-maxillary fixation (IMF) was released. Occlusion was re-assessed on opening and closing the mouth, which was found to be satisfactory. The patient recovered well from the anaesthesia and was moved to post-operative ICU.
Post-surgical procedure
The patient was asked to maintain the appliance for the next year to check for the stability of treatment. During this phase, continuous 0.016″ Ni-Ti and 0.018″ stainless steel wires were placed and dento-alveolar expansion was performed with the wire. Elastics were given to close the bite and for the correction of midline. After this, the appliance was debonded and a fixed lingual retainer was bonded in the lower arch and a removable Hawley's retainer with posterior bite plane was used in the upper arch. The patient was advised to extract the third molars.
Results
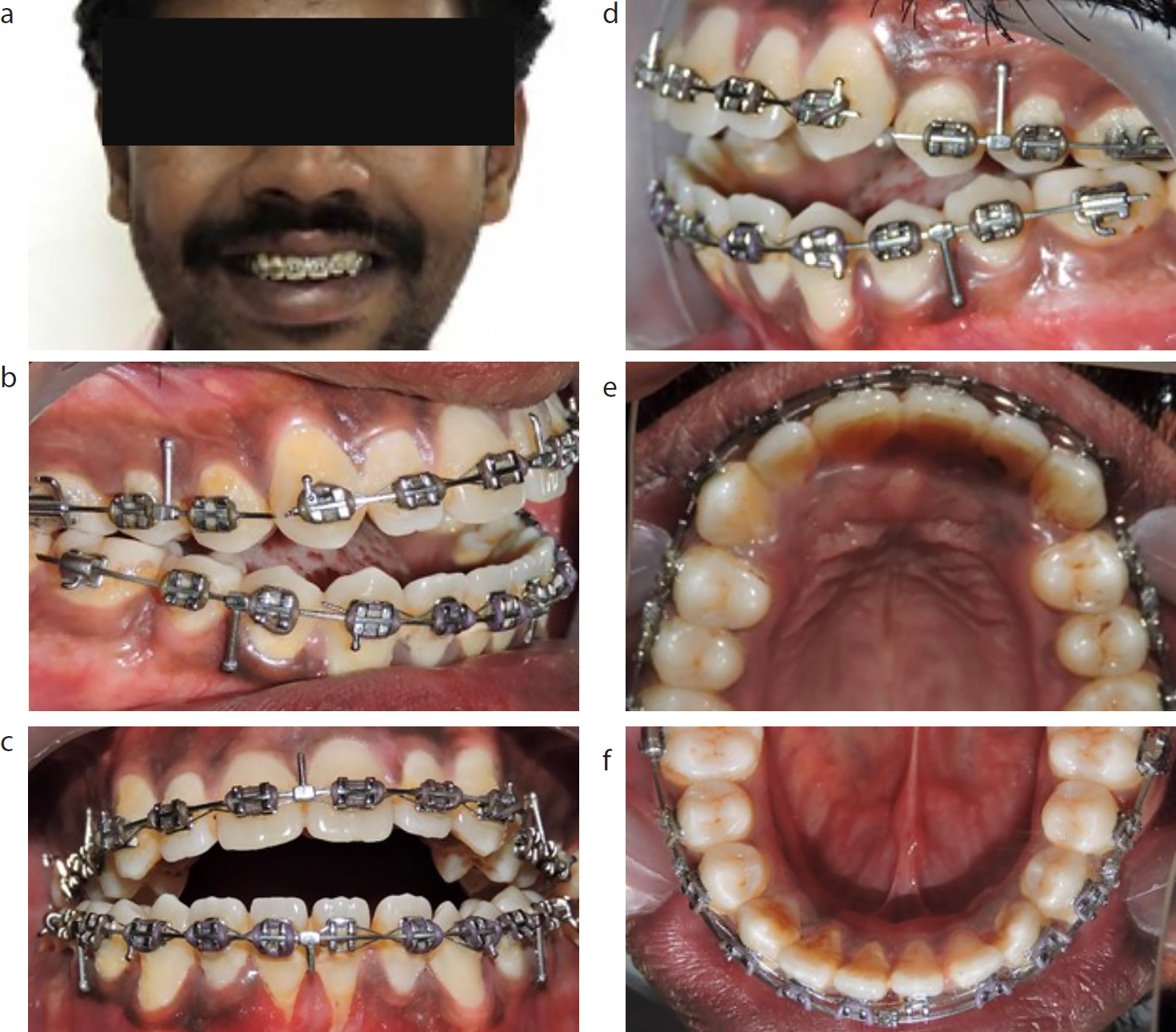
Treatment time was 1 year and 10 months. At the end of the treatment, a proper overjet and overbite with improvement in appearance as well as function was achieved (Figure 5). The patient reported an improvement in bite.
Figure 5.
(a–f) Post-treatment views.
Discussion
Over the years, orthodontics gives special attention to vertical facial proportions. However, vertical malocclusions are difficult to treat, often with unstable results. Taking this into consideration, it is better to treat vertical problems with a combination of orthodontics and orthognathic surgery.3,4 Correction of skeletal problems can help to improve a patient's psychology and may lead to a better result.
While doing molar intrusion with implants or surgery, it is important to check the incisor exposure at rest and the smile pre-treatment. Patients with insufficient incisor exposure with conventional incisor extrusion should be treated with elastics.5
Previous studies have shown stability in the treatment of skeletal open bite by Le Fort I and bilateral sagittal split osteotomy. The results were maintained 15 years after surgery.6 Hoppenreijs suggested that patients treated with a Le Fort I osteotomy, in one-piece or in multi-segments, with or without bilateral sagittal split osteotomy, showed good results long term.7 Posterior Le Fort I impaction, as well as anterior extrusion, with or without bilateral sagittal split osteotomy, also show good results post-surgery.8 In our case, posterior asymmetric impaction was planned, with mild box elastic wear post-surgery. The posterior impaction led to counter-clockwise rotation of the mandible and improved the appearance of the patient.
As tongue posture and size play an important role in the aetiology of the open bite, partial glossectomy is acceptable for cases with open bite and macroglossia.9,10 In this case, the tongue thrust habit was intercepted by motivating the patient to perform elastic swallow exercises. At the end of treatment, the patient was content with the results overall.
Conclusions
Severe anterior open bites can be treated successfully with posterior impaction by Lefort 1 osteotomy.