Fleming PS, Marinho V, Johal A Orthodontic measurements on digital study models compared with plaster models: a systematic review. Orthod Craniofac Res. 2011; 14:1-16
Assessment of the reliability of measurements taken on digital orthodontic models obtained from scans of plaster models in laboratory scanners. A systematic review and meta-analysis. 2022. https://doi.org/10.1093/EJO/CJAC005
Goracci C, Franchi L, Vichi A, Ferrari M Accuracy, reliability, and efficiency of intraoral scanners for full-arch impressions: a systematic review of the clinical evidence. Eur J Orthod. 2016; 38:422-428
Rossini G, Parrini S, Castroflorio T Diagnostic accuracy and measurement sensitivity of digital models for orthodontic purposes: a systematic review. Am J Orthod Dentofac Orthop. 2016; 149:161-170
Rangel FA, Chiu YT, Maal TJJ Does powdering of the dentition increase the accuracy of fusing 3D stereophotographs and digital dental casts. Eur J Orthod. 2016; 38:440-445
Grünheid T, McCarthy SD, Larson BE Clinical use of a direct chairside oral scanner: an assessment of accuracy, time, and patient acceptance. Am J Orthod Dentofac Orthop. 2014; 146:673-682
Kang SJ, Kee YJ, Lee KC Effect of the presence of orthodontic brackets on intraoral scans. Angle Orthod. 2021; 91:98-104
Sohmura YH, Satoh H, Takahashi J, Takada K Complete 3-D reconstruction of dental cast shape using perceptual grouping. IEEE Trans Med Imaging. 2001; 20:1093-1101
Schirmer UR, Wiltshire WA Manual and computer-aided space analysis: a comparative study. Am J Orthod Dentofacial Orthop. 1997; 112:676-680
Murugesan A, Sivakumar A Comparison of accuracy of mesiodistal tooth measurements made in conventional study models and digital models obtained from intraoral scan and desktop scan of study models. 2020; 47:149-155 https://doi.org/10.1177/1465312520910755
Porter JL, Carrico CK, Lindauer SJ, Tüfekçi E Comparison of intraoral and extraoral scanners on the accuracy of digital model articulation. 2018; 45:275-282 https://doi.org/10.1080/1465312520181500773
Christopoulou I, Kaklamanos EG, Makrygiannakis MA Patient-reported experiences and preferences with intraoral scanners: a systematic review. Eur J Orthod. 2022; 44:56-65
Burhardt L, Livas C, Kerdijk W Treatment comfort, time perception, and preference for conventional and digital impression techniques: a comparative study in young patients. Am J Orthod Dentofac Orthop. 2016; 150:261-267
Burzynski JA, Firestone AR, Beck FM Comparison of digital intraoral scanners and alginate impressions: time and patient satisfaction. Am J Orthod Dentofac Orthop. 2018; 153:534-541
Glisic O, Hoejbjerre L, Sonnesen L A comparison of patient experience, chair-side time, accuracy of dental arch measurements and costs of acquisition of dental models. Angle Orthod. 2019; 89:868-875
Yilmaz H, Özlü FÇ, Karadeniz C, Karadeniz EI Efficiency and accuracy of three-dimensional models versus dental casts: a clinical study. Turkish J Orthod. 2019; 32
Computerized casts for orthodontic purpose using powder-free intraoral scanners: accuracy, execution time, and patient feedback. 2018. https://doi.org/10.1155/2018/4103232
Patzelt SBM, Lamprinos C, Stampf S, Att W The time efficiency of intraoral scanners. J Am Dent Assoc. 2014; 145:542-551
Joda T, Brägger U Patient-centered outcomes comparing digital and conventional implant impression procedures: a randomized crossover trial. Clin Oral Implants Res. 2016; 27:e185-e189
Luqmani S, Jones A, Andiappan M, Cobourne MT A comparison of conventional vs automated digital peer assessment rating scoring using the Carestream 3600 scanner and CS Model+ software system: a randomized controlled trial. Am J Orthod Dentofac Orthop. 2020; 157:148-155.e1.
Kapila SD, Nervina JM CBCT in orthodontics: assessment of treatment outcomes and indications for its use. Dentomaxillofac Radiol. 2015; 44 https://doi.org/10.1259/dmfr.20140282
Jacox LA, Bocklage C, Edwards T Understanding technology adoption by orthodontists: a quantitative study. Am J Orthod Dentofac Orthop. 2022; 161:364-374
Tartaglia GM, Mapelli A, Maspero C Direct 3D printing of clear orthodontic aligners: current state and future possibilities. Materials (Basel). 2021; 14 https://doi.org/10.3390/ma14071799
Koenig N, Choi JY, McCray J Comparison of dimensional accuracy between direct-printed and thermoformed aligners. Korean J Orthod. 2022; 52:249-257
The landscape of orthodontics is changing, and the transition to digital workflows in clinical practice has begun. As new and updated scanner models are regularly being released, it is paramount to assess the current evidence base and compare this to manufacturer claims. At present, there are limited literature reviews assessing and summarizing the clinically relevant features of dental scanners. This review summarizes key findings with respect to accuracy, patient-related outcomes and clinician experiences with digital dental scanners.
CPD/Clinical Relevance: Digital scanners are an increasingly popular device in orthodontics, this article provides an up-to-date summary of the pros and cons of scanners in relation to both the patient and orthodontic clinician.
Article
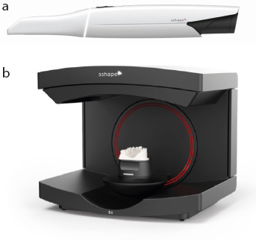
Both intra-oral scanners and extra-oral laboratory scanners are gradually replacing conventional methods of diagnosis and treatment planning (Figure 1). Digital scanning has several advantages over its analogue counterparts, including reduced need for physical storage of casts, transferable data for communication with patients and other dental professionals, and the ability to visualize three-dimensional (3D) models almost instantly. However, they are not without drawbacks, some of which include expensive set-up and maintenance costs, and a significant learning curve for all those involved in adopting the technology.
Figure 1. A visual depiction of the different appearances between (a) intra-oral (TRIOS 5, 3Shape, Copenhagen, Denmark) and (b) extra-oral (E4 Lab Scanner, 3Shape, Copenhagen, Denmark) scanners.
Accuracy of dental scanners
Alginate impressions taken for the construction of plaster casts are the most common method used in clinical practice, aiding in orthodontic treatment planning. These are currently still accepted as the gold standard,1 but these come with significant disadvantages such as model damage, transport and pouring inaccuracies, as well as time taken to fabricate models and the subsequent need for storage. As of May 2023, the NHS Records Management Code of Practice recommends that clinical dental records be kept for at least 11 years.2 With recent developments and reductions in costs of dental scanners, there has been an increase in popularity of virtual models. However, for a patient's occlusion to be correctly assessed, and for teeth to be moved predictably and effectively, it is imperative that the models we use are accurate.
As optical technology advances, both scanning accuracy and efficiency will improve. Intra-oral scanners produce a scan in three stages:
Image capture;
Data processing;
Presentation of results onscreen.
An intra-oral scanner may use confocal laser scanning in which a laser is emitted through a pinhole filter to only allow one focal plane to be focused on the scanner's sensor. Anything out of focus is not recorded and the process is repeated until the computer software develops a 3D scan from the 2D images. This process is known as ‘point-and-stitch reconstruction’, and both iTero (Align Technology, CA, USA) and TRIOS (3Shape, Copenhagen, Denmark) scanners use this method. Other techniques, such as triangulation and active wave-front sampling, are also used in intra-oral scanners; however, application of a thin layer of powder is required. The current evidence on scanning accuracy is sparse, and as progress in the field continues and new models of scanners are released, there is a requirement to assess their reliability and validity.
One systematic review assessed the accuracy of extra-oral scaners and compared them to conventional impressions.3 Nine studies met the inclusion criteria, but all articles were of low quality and displayed significant heterogeneity. The authors noted that the various models of scanners of differing brands and software presented challenges during comparisons of their accuracy. There was a distinct lack of information regarding demographics, with only one paper including age of participants. Deciduous and mixed dentitions were excluded and measurements of accuracy between studies were not standardized. The review concluded that there were no clinically relevant differences between the accuracy of analogue and digital methods. However, owing to the limitations discussed in the paper, further high-quality evidence is required to provide valid conclusions.
Another systematic review assessed the accuracy of intra-oral scanners as a form of digital impression-taking.4 In this review, accuracy was described as the closeness of software measurements on digital models when compared with calliper measurements on stone casts. Only half of the papers assessed reproducibility, validity and repeatability, but found that intra-oral scanners were comparable to analogue impressions. These results were supported by a further paper that showed high accuracy and reproducibility of digital models and even went on to say that they could be considered the new gold standard.5 Both papers admitted that there were significant limitations, for example, the studies that met the search criteria in Goracci et al's systematic review were limited to complete permanent dentition from first molar to first molar.4 Although this reduced heterogeneity of the sample, children were excluded. Children make up a large proportion of the orthodontic patient base and, therefore, it would be prudent to consider factors that may alter scanning accuracy, such as missing teeth, mobile deciduous teeth, differing size of teeth and patient compliance.
Accuracy of intra-oral scanners can be affected by the light that reflects off the shiny surfaces of teeth. To mitigate this problem, powder can be placed on tooth surfaces prior to scanning. A prospective study assessed the effects of powdering on scan accuracy and compared this to non-powdered dentitions.6 A titanium-dioxide powder spray was used and the sample consisted of 20 residents from the department of orthodontics and craniofacial biology at Radboud University Medical Centre in the Netherlands. None of the participants had severe malocclusions. This sample may have introduced bias as orthodontic residents may have been easier to scan owing to good compliance and lack of malocclusion. The authors concluded that powdering had a statistically significant benefit, but the difference in accuracy was <0.1 mm and therefore had minimal clinical relevance.
Additionally, it is important to acknowledge the effect this has on clinician- and patient-related outcomes. Powdering teeth may slightly improve accuracy, but it may decrease the efficiency of scanning and reduce patient comfort owing to the resulting dry mouth.6 Another study that compared alginate impressions to prepowdered intra-oral scanners found that 40% of patients found the scan somewhat uncomfortable.7 However, there are limited data on patient-related outcomes, suggesting the need for further assessment to investigate patient experience when powdering the dentition.
Intra-oral scanners provide clinicians with an opportunity to perform scans mid-treatment to assess progress. However, intra-oral scanners must allow for accurate scanning with fixed appliances in situ, as reflections may alter scanning accuracy. Kang et al analysed the effect of this on 30 patients using iTero and TRIOS intra-oral scanners.8 They concluded that presence or absence of brackets did not affect overall dimensions of teeth and that scans were clinically acceptable for orthodontic treatment planning. This was based on the fact that all 3D images, with and without brackets, had errors of <0.30 mm. Hirogaki et al suggested that an orthodontic diagnostic model is clinically useful if its accuracy is approximately within 0.30 mm. Conversely, Schirmer et al stated that errors should be no more than 0.20 mm.9,10 To date, there is no absolute value for what amount of deviation is acceptable, but considerations on clinical significance should be stated.
A drawback of intra-oral scanners is that patient anatomy and saliva can affect image quality. One prospective study compared the accuracy of mesiodistal tooth measurements of digital models from both extra- and intra-oral scans.11 They concluded that there were statistically significant differences in the accuracy of both scanning methods, but a limited sample size of only 10 patients was used. A second study also compared the different digital dental scanners and specifically assessed accuracy of model articulation.12 It is important that both intra-and inter-arch accuracy is correctly recorded during scanning as assessment of the molar and canine relationship, overbite and overjet are dependent on correctly articulated models. Of the scanners tested, the authors found that only iTero and iTero Element scanners produced inter-arch measurements within a range of ±0.5 mm.
Summary for accuracy
Up-to-date studies with improved trial design are required to evaluate the accuracy of dental scanners. Currently there is limited evidence to confidently state that scanning is more accurate than conventional impression-taking. There is limited information regarding intra-oral scanner use in children with malocclusions, and much of the data on scanning accuracy comes from different brands of scanners and software. It is therefore our recommendation that future papers incorporate patients in the mixed dentition and aim to use the same brand of scanner to reduce selection bias and improve external validity. Following the review of the literature, it can also be suggested that intra-oral scanners should be assessed on patients who present with complex malocclusions so that findings can be comparable to our sample population.
Patient-reported experiences of intra-oral scanners
Analysis of patient-reported experiences of intra-oral scanners is less welldocumented than scanning accuracy. Our patients should be central to the treatment we provide and assessing the patient experience can allow clinicians to develop personalized treatment plans. Additionally understanding the patient perspective could also help intra-oral scanner manufacturers to improve their products.
One systematic review compared nine high-quality studies that looked at patient-reported experiences and preferences regarding intra-oral scanners.13 Eight of the nine studies reported a general trend of patients preferring intra-oral scanners over conventional impression materials. By contrast, another study showed that 73% of patients preferred alginate impressions over intra-oral scanners (Lava COS, 3M ESPE, St Paul, MN, USA) as they were said to be ‘easier’ and ‘faster’.7 However, this may have been due to the application of titanium dioxide powder prior to the scan, which modern scanners do not require. Additionally, Burhardt et al suggested there was a risk of bias with this conclusion owing to a lack of a ‘washout period’ between patient experiences. Washout periods are required when individuals within a crossover trial undergo multiple different clinical treatments/trials within a single study, so require a period of no treatment to ensure that one method does not impact the data of the next. As there was no evidence of such a period, the data could have been skewed towards one modality, thus decreasing its internal validity.13,14
Intra-oral scanner comfort
The comfort of digital scanners is possibly the most important patient-related factor to consider. Burhardt et al reported that 51% of patients within their study preferred intra-oral scanners over alginate impressions. Specifically, participants felt more comfortable with the CEREC Omnicam (Sirona Dental Systems, Bensheim, Germany) scanner than with the Lava Chairside Oral Scanner.14 In a later study, Burzynski et al also concluded that intra-oral scanners were more comfortable, but highlighted that there was a statistically significant difference in comfort between the iTero Element intra-oral scanner, and the TRIOS Color scanner, reporting the former had superior comfort.15 That said, studies that specifically analysed use of the TRIOS scanner still showed increased comfort compared to conventional alginate material.16,17,18
Time perception and chairside time
Time perception has been a topic of controversy in the literature, as the subjective opinion of how long intra-oral scanning takes in relation to conventional impression techniques is thought to be directly related to patient expectations, previous experiences and comfort.15 Interestingly six out of the nine studies reviewed by Christopoulou et al showed that time perception for intra-oral scanners was shorter than for alginate, despite longer objective chairside time.13 The other studies in the systematic review showed no statistical difference in the perception of time taken to complete impressions with conventional methods and different types of scanners. The Lava Chairside Oral Scanner was shown to have taken the longest chairside time, owing to a need to apply powder and take three separate scans for each arch, along with an inter-occlusal record. However, with the advent of powder-free intra-oral scanners, and the rapid development of software, this finding may not be representative of current scanning times. Furthermore, operator skill and familiarity play a large role in the speed of the scan, chairside time and patient experience, which can also act as confounding factors when considering the patient's perception of time.
Burhardt et al found the difference in average chairside time for intra-oral scanners and alginate impressions was not statistically significant;14 alginate took a total of 9.72 minutes when compared to the Lava Chairside Oral Scanner and CEREC Omnicam, which took 17.83 minutes and 10.47 minutes respectively.14 Burzynski et al showed similar times, with alginate taking 6.4 minutes, iTero intra-oral scanners taking 7 minutes and TRIOS intra-oral scanners taking 8.6 minutes.15 However, the literature is inconsistent because there are other variables that affect chairside time, such as difference in operator skill and experience, as well as the number of scans/impressions required, and the type of intra-oral scanner or alginate used. One study showed that the iTero scanner had a mean intra-oral time of 7 minutes 55 seconds, while the total chairside time, including use of software was approximately 20 minutes 17 seconds. Moreover, the Lava Chairside Oral Scanner had an average intra-oral time of 10 minutes 51 seconds, while the total cumulative chairtime was 17 minutes 20 seconds.19 It is evident that there is a lack of consistency as to what defines chairside time, hence there is no current consensus that scanning is faster than conventional impressions, nor is there a particular intra-oral scanner that has been proven to be more time efficient.
Other markers and patient-related outcomes
Triggering the gag reflex during conventional impression-taking is a common occurrence, even when the patient is not hyper-responsive. One study found no significant statistical differences in provoking gag reflexes. Despite this, the results indicated that total perception scores of intra-oral scanners, which include gag reflex, queasiness and breathing issues, were more favourable in comparison to alginate impressions.14
Other patient-reported outcomes, such as sensation in terms of taste, vibrations, heat, smell as well as temporomandibular joint discomfort were suggestive of greater positive experiences when intra-oral scanners were used.13 Joda et al used a 100-mm visual analogue scale to measure bad taste across 20 patients who received intra-oral scans and conventional impressions. They found the mean value for intra-oral scanners was 10.9 while conventional impressions received a mean value of 71.3.20 Another study, also using visual analogue scales, agreed with this conclusion, showing a significant difference between the two treatment modalities.16 However, studies with higher-quality evidence are required to clearly identify whether there are any clinically significant differences for these patient-reported outcome measures.
Table 1. Summary of the domains reported in the literature when comparing intra-oral scanning to conventional alginate impressions.
Area of interest
Summary
Clinician factors
Accuracy
Limited high-quality evidence to show that intra-oral scanning is more accurate than alginate for orthodontic purposes, particularly in children with more challenging malocclusions
Efficiency and chairside time
Conflicting results: when compared to alginate, evidence currently shows intra-oral scanning takes more total chairside time. NB some evidence includes time to apply powder, which is no longer relevant with current intra-oral scanners
Patient factors
General preference
Intra-oral scanning has been shown to be preferred by patients over conventional alginate impressions
Comfort
Intra-oral scanning has been shown to be more comfortable than conventional alginate impressions
Time perception
Patients reported that intra-oral scanning was perceived as a quicker procedure than conventional alginate impressions, despite taking longer in objective chairside time
Gag reflex
Patients reported less gagging with intra-oral scanning when compared to conventional impressions
Taste
Patients do not find intra-oral scanning as offensive in taste compared with conventional impressions
TMJ disorders
Patient reported outcomes show that there is no significant difference between conventional impressions and intra-oral scanning in relation to the incidence of temporomandibular joint disorders
Summary for patient-related factors
Further high-quality evidence is required to compare the intra-oral scanners against a control, such as alginate. The available literature seems to have used multi-generational scanners at different points in time and no single study has demonstrated a comparison of up-to-date scanners. Further research comparing several new powder-free scanners could help to differentiate between intra-oral scanners in terms of their contribution to improving clinical practice, as well as producing further high-quality evidence. Once such studies are complete, their impact on patient--related outcomes can be clearly assessed and defined.
Clinician-related factors
Efficiency and chairside time
As previously mentioned, the current literature suggests that conventional impressions are still more time efficient than intra-oral scanning.14,15 However, these results are difficult to interpret owing to lack of clarity in defining chairside time. The generalizability of previous research is limited due to developments in scanning technology and varied clinician experience. Most clinicians feel more confident and are more experienced with conventional impressions compared to intra-oral scanning. Differences in clinician experience could be considered a confounding factor when assessing chairside time, potentially explaining the large inconsistencies in scanning efficiency. In addition to this, the complexity of the software or demands of the scanner may add to total time taken.13,14 Studies published in implant and prosthetic journals have shown faster chairside times with intra-oral scanners. For example, Patzelt et al suggested that chairside time was lower with intra-oral scanners when compared to taking impressions for abutment teeth in prosthetics.19 However, studies such as these may not be as relevant in the orthodontic field, as full arch scanning is required and the common impression material of choice for orthodontic study models is usually a fast-setting alginate rather than a polyvinyl siloxane or polyether. Further studies assessing full arch scans and comparing them to alginate impressions are required to highlight any clinically significant difference between the two modalities of record taking.
A further limitation in many previous studies was discrepancies in what was considered scanning time. The evidence was unclear as to whether cotton wool placement, powdering and bite registration was included in the time taken for scans. In addition, use of software and time to set up an intra-oral scanner should all contribute to total chairside time. Additional information is required with experienced clinicians to provide a clearer comparison of total chairside times, considering all necessary work carried out prior to and after the scan itself. Furthermore, time for re-scanning and re-taking impressions should also be included within future studies because this would be more representative of the true chairside time required to create a clinically acceptable record.
Peer assessment rating and other potential uses for scanners
Peer assessment rating is a form of treatment outcome assessment carried out by orthodontists in the UK to objectively determine the impact of orthodontic treatment on the initial malocclusion, by comparing initial and final records of NHS cases. Luqmani et al compared how the use of intra-oral scanners and conventional methods (alginate impressions cast up in plaster) affected the peer assessment score. The study reported that no statistically significant difference was found. However, there is scope to use scanner software to measure digital models, and this has the potential to provide clinically improved outcomes when compared with conventional methods.21
Another potential use for scanners is space analysis. According to Yilmaz et al, intra-oral scanning is more time efficient when carrying out space analysis.17 Although the intentions in this study were positive, confounding factors and limited external validity mean that the conclusions may be difficult to extrapolate. Therefore further high-quality studies and systematic reviews are required to provide clarity on whether space analysis and Bolton discrepancy analysis is better with casts or scans, and whether any clinical or statistical significance exists.
Summary of clinician-related factors
Overall, there is positive indication that intra-oral scanners provide benefits to clinicians; however, it is not yet possible to draw clear conclusions given the lack of high-quality evidence. It is likely that as intra-oral scanners become more popular, more relevant and generalizable studies will become available.
The future of scanners in orthodontics
Intra- and extra-oral scanners are a growing trend in orthodontics, highlighting the increasing development of digital technology in dentistry. Another dental technological breakthrough is the use of cone beam computed tomography (CBCT). Since its introduction in 1998, CBCT has been used in orthodontics to aid diagnosis, treatment planning and research. Its increase in popularity is mainly a result of the advantages that 3D imaging has over 2D imaging. CBCT is currently indicated in orthodontics in cases of impacted teeth, cleft lip and palate, and skeletal discrepancies requiring surgical intervention.22
Currently, some dental scanning software can superimpose the 3D models extrapolated from an intra-oral scan with the data from a CBCT. This combined image provides the clinician with an accurate digital model of both the crowns and roots of teeth. Align Technology has recently integrated CBCT into their ClinCheck Pro 6.0 software, claiming that this allows a clinician to be more confident and comprehensive in their treatment planning.23 Although the combination of data from radiographs, intra-oral scanning and photography can lead to more accurate diagnoses and improved treatment planning, it is important to ensure that the use of CBCT is justified, and any benefits should outweigh the risks of the imaging.22
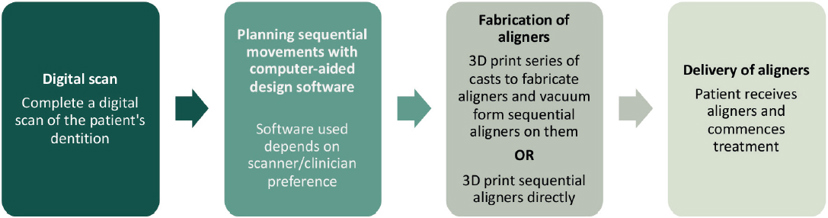
In-house aligner fabrication, in which scanners have an integral role, is another exciting prospect in orthodontics. The process of creating aligners (Figure 2) uses additive manufacturing, more commonly known as 3D printing. One of the main benefits of in-house aligners is reduced expenditure. It is significantly cheaper to fabricate aligners in-house than to outsource to commercial companies, and this saving can be passed on to patients. There is also the benefit of efficiency. For example, once treatment is planned, patients can start a course of aligners the following day and any lost or broken aligners can be easily replaced. Moreover, it provides a greater level of control for clinicians. However, the process is time consuming and labour intensive, and the upfront cost of equipment is high. There is also a requirement for purchasing software and subscriptions, which increases costs further. Additionally, there is a significant learning curve for staff to overcome, and time would be required for the adoption of any technological advances. These are all boundaries to technology adoption and as shown in a qualitative study, ease of implementation is one of the key adoption incentives.24
Figure 2. A flow diagram illustrating the design and manufacturing process for in-house aligners.
Recent developments have led to directly 3D-printed clear aligners, which may negate the need for the vacuum forming process, and allows for material to be selectively added onto aligners in specific areas, for example to create bite planes.25 Also, there is new evidence to show that directly 3D-printed aligners have greater dimensional accuracy in comparison to thermoformed counterparts.26
Conclusions
Digital scanning in dentistry is becoming increasingly popular, but there is still a lack of high-quality evidence in patient- and operatorreported outcomes. However, both patients and clinicians generally approve of its use, and the current evidence suggests that it is a valid and accurate alternative for orthodontic diagnosis and treatment planning.