Chockattu SJ, Suryakant DB, Thakur S. Unwanted effects due to interactions between dental materials and magnetic resonance imaging: a review of the literature. Restor Dent Endod. 2018; 43
Hasanin M, Kaplan SEF, Hohlen B, Lai C, Nagshabandi R, Zhu X, Al-Jewair T. Effects of orthodontic appliances on the diagnostic capability of magnetic resonance imaging in the head and neck region: a systematic review. Int Orthod. 2019; 17:403-414
Görgülü S, Ayyıldız S, Kamburoğlu K, Gökçe S, Ozen T. Effect of orthodontic brackets and different wires on radiofrequency heating and magnetic field interactions during 3-T MRI. Dentomaxillofac Rad. 2014; 43
Mir AP, Rahmati-Kamel M. hould the orthodontic brackets always be removed prior to magnetic resonance imaging (MRI)?. J Oral Biol Craniofac Res. 2016; 6:142-152
Zachriat C, Asbach P, Blankenstein KI, Peroz I, Blankenstein FH. MRI with intraoral orthodontic appliance—a comparative in vitro and in vivo study of image artefacts at 1.5T. Dentomaxillofac Rad. 2015; 44
Kemper J, Priest AN, Schulze D, Kahl-Nieke B, Adam G, Klocke A. Orthodontic springs and auxiliary appliances: assessment of magnetic field interactions associated with 1.5 T and 3 T magnetic resonance systems. Eur Radiol. 2007; 17:533-540
Ozawa E, Honda E, Parakonthun KN, Ohmori H, Shimazaki K, Kurabayashi T, Ono T. Influence of orthodontic appliance-derived artifacts on 3-T MRI movies. Prog Orthod. 2018; 19
Zhylich D, Krishnan P, Muthusami P, Rayner T, Shroff M, Doria A, Tompson B, Lou W, Suri S. Effects of orthodontic appliances on the diagnostic quality of magnetic resonance images of the head. Am J Orthod Dentofac. 2017; 151:484-499
Hasegawa M, Miyata K, Abe Y, Ishigami T. Radiofrequency heating of metallic dental devices during 3.0 T MRI. Dentomaxillofac Radiol. 2013; 42
Sadowsky PL, Bernreuter W, Lakshminarayanan AV, Kenney P. Orthodontic appliances and magnetic resonance imaging of the brain and temporomandibular joint. Angle Orthod. 1988; 58:9-20
Wylenzinska M, Pinkstone M, Hay N, Scott AD, Birch MJ, Miquel ME. Impact of orthodontic appliances on the quality of craniofacial anatomical magnetic resonance imaging and real-time speech imaging. Eur J Orthod. 2015; 37:610-617
Sung JW, Kwon TY, Kyung HM. Debonding forces of three different customized bases of a lingual bracket system. Korean J Orthod. 2013; 43:235-241
Klocke A, Kahl-Nieke B, Adam G, Kemper J. Magnetic forces on orthodontic wires in high field magnetic resonance imaging (MRI) at 3 Tesla. J Orofac Orthop. 2006; 67:424-429
Kajan ZD, Khademi J, Alizadeh A, Babaei Hemmaty Y, Atrkar Roushan Z. A comparative study of metal artifacts from common metal orthodontic brackets in magnetic resonance imaging. Imaging Sci Dent. 2015; 45:159-168
Sinkiewicz D. MRI scan hazard. Br Dent J. 2013; 214
Erasmus LJ, Hurter D, Naudé M, Kritzinger HG, Acho S. A short overview of MRI artefacts. S Afr J Radiol. 2004; 8:13-17
Blankenstein FH, Asbach P, Beuer F, Glienke J, Mayer S, Zachriat C. Magnetic permeability as a predictor of the artefact size caused by orthodontic appliances at 1.5 T magnetic resonance imaging. Clin Oral Investig. 2017; 21:281-289
Tymofiyeva O, Vaegler S, Rottner K, Boldt J, Hopfgartner AJ, Proff PC, Richter E, Jakob PM. Influence of dental materials on dental MRI. Dentomaxillofac Rad. 2013; 42
Costa AL, Yasuda C, Appenzeller S. Artifacts in brain magnetic resonance imaging due to metallic dental objects. Med Oral Patol Oral Cir Bucal. 2009; 14:278-282
Hunt HL. Orthodontic appliances and MRIs. Am J Orthod Dentofacial Orthop. 2009; 135
Cassetta M, Pranno N, Stasolla A, Orsogna N, Fierro D, Cavallini C, Cantisani V. The effects of a common stainless steel orthodontic bracket on the diagnostic quality of cranial and cervical 3T – MR images: a prospective, case-control study. Dentomaxillofac Rad. 2017; 46
Okano Y, Yamashiro M, Kaneda T, Kasai K. Magnetic resonance imaging diagnosis of the temporomandibular joint in patients with orthodontic appliances. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003; 95:255-263
Patel A, Bhavra GS, O'Neill JR. MRI scanning and orthodontics. J Orthod. 2006; 3:246-249
Beau A, Bossard D, Gebeile-Chauty S. Magnetic resonance imaging artefacts and fixed orthodontic attachments. Eur J Orthod. 2014; 37:105-110
Elison JM, Leggitt VL, Thomson M, Oyoyo U, Wycliffe ND. Influence of common orthodontic appliances on the diagnostic quality of cranial magnetic resonance images. Am J Orthod Dentofac. 2008; 134:563-572
Ul-Haq A, Ul-Hamid MW, Jafri AR. To determine mean distortion score of MRI at nine different sections of head and neck with dantauram metallic orthodontic brackets on the teeth. Pak Oral Dent J. 2015; 35
Cox RJ, Kau CH, Rasche V. Three-dimensional ultrashort echo magnetic resonance imaging of orthodontic appliances in the natural dentition. Am J Orthod Dentofac. 2012; 142:552-561
Harris TMJ, Faridrad MR, Dickson JAS. The benefits of aesthetic orthodontic brackets in patients requiring multiple MRI scanning. J Orthod. 2006; 33:90-94
Aizenbud D, Hazan-Molina H, Einy S, Goldsher D. Craniofacial magnetic resonance imagine with a gold solder-filled chain-like wire fixed orthodontic retainer. J Craniofac Surg. 2012; 23:e654-e657
Shalish M, Dykstein N, Friedlander-Barenboim S, Ben-David E, Gomori JM, Chaushu S. Influence of common fixed retainers on the diagnostic quality of cranial magnetic resonance images. Am J Orthod Dentofacial Orthop. 2015; 147:604-609
Magnetic resonance imaging (MRI) uses strong magnetic fields, magnetic gradients and radio waves to produce images of the body. The demand for MRI is steadily increasing as it does not use ionizing radiation and has excellent soft tissue contrast. Certain materials used in components of fixed orthodontic appliances can cause unwanted effects and affect the diagnostic quality of MR images by producing artefacts. This article proposes an evidence-based protocol that aims to standardize the management of orthodontic patients undergoing MRI scans.
CPD/Clinical Relevance: As the use of MRI continues to increase, it is becoming more likely that orthodontists will encounter patients requiring MRI scans of the head and neck region during the course of their orthodontic treatment.
Article
The effects of dental materials on Magnetic Resonance Imaging (MRI) have long been studied. Many materials, including certain components of fixed orthodontic appliances, can cause unwanted effects such as radiofrequency-induced heating, magnetically-induced displacement and artefact formation when placed in MRI scanners; this can result in inaccurate diagnoses and treatment.1 An onus is therefore placed on the orthodontist to decide which components should be removed before their patients undergo MRI scans. There are currently no guidelines or protocols available to facilitate this decision, and often, all components are removed prior to the investigation taking place.2,3,4,5 This can be costly and time-consuming, lengthen treatment time and cause enamel damage.4,5,6,7,8 An increasing number of orthodontic patients who require MRI scans are presenting at Cardiff Dental Hospital. A need was identified for an evidence-based protocol that aids the clinician in the management of these patients.
Methodology
An initial scoping search was carried out using an internet search engine (Google) to check for existing protocols; none was found. Following this, a literature search was performed using five well-known databases (Pubmed, Ovid, Google Scholar, Clinical Key and Research Gate) with the following keywords: orthodontic appliances; magnetic resonance imaging; MRI; unwanted effects; artefacts/artifacts. In total, 27 relevant abstracts were identified, which consisted of 20 case–control studies, one cross-sectional study, two literature reviews, one case report, two letters to the editor and one systematic review and meta-analysis. The results were used to formulate a protocol.
Results
Three effects can occur as a result of placing fixed orthodontic components in MRI scanners: radiofrequency-induced heating, magnetically induced displacement and artefact formation.1 These are discussed below and summarized in Table 1. Other factors to consider include the anatomical region being imaged and the MRI sequence used.
Effect type
Findings
Physical effects: radiofrequency-induced heating
The temperature increase of components of fixed orthodontic appliances is generally regarded as insufficient to cause pain or damage to periodontal tissues.1,2One study by Hasegawa et al stated that stainless steel arch wires may exhibit heating above acceptable levels and recommended the removal of this type of archwire prior to scanning.10
Components of fixed orthodontic appliances are safe to use in MRI scanners when firmly bonded and carefully ligated.4,5,6,11,12 Hunt suggested the fabrication of Essix trays to secure retainers and fixed attachments.21Removable and/or loose components and appliances should be removed prior to scanning.4,6,11,12Görgülü et al deemed brackets to be ‘MR safe’ but stated that stainless steel and nickel–titanium wires pose a potential risk. They therefore recommended their removal prior to scanning.2
Artefact formation
The severity and extent of artefact formation is dependent on the magnetic properties of the metal object; distance from the region being imaged; the shape, position, orientation and number of objects; the homogeneity of the alloy and the MRI sequence and sequence parameters used.1,4,7,11,18,19Archwires: stainless steel archwires can cause artefacts that render an MRI scan of the head and neck region non-diagnostic.4,12,15,19,22,23,24 Ceramic archwires cause minimal artefacts.23Brackets: stainless steel brackets can cause artefacts that render MRI scans of the head and neck region non-diagnostic.4,8,12,19,22,23,25,26,27 Ceramic brackets with stainless steel slots can cause significant artefacts if the area of interest is within the oral cavity.4,25,28,29 Ceramic and plastic brackets cause minimal to no artefacts.5,8,12,23,25,26,27,28 Further research is required on titanium brackets as differing opinions exist: some authors concluded that they cause minimal artefacts,4,26 whereas others stated that they can cause artefacts if the area of interest is within the oral cavity.1,25Bonded retainers: stainless steel bonded retainers can cause unacceptable artefacts if the area of interest is within the oral cavity.4,25 Bonded retainers fabricated from gold solder-filled wire (such as Ortho Flex Tech) appear not to cause artefacts in MRI scans of the head and neck and may not need to be removed prior to an MRI investigation.30,31 Further research is required on nickel–titanium retainers. As nickel is an extremely ferromagnetic material known to cause large artefacts,1,15 it may be pertinent to remove nickel–titanium bonded retainers prior to MRI scans of the head and neck region.
Anatomical region of interest
In general, the closer the metallic object to the anatomical region being imaged, the greater the signal loss and image distortion.4,8,11,26Further research is required on the effects of fixed orthodontic appliances on defined anatomical regions of head and neck MR images.
Physical effects: radiofrequency-induced heating
Magnetic radiofrequency fields employed during MRI scans can induce electrical currents in metallic objects. The resultant thermal heating can cause localized tissue damage and lead to dysfunction of implanted medical devices.9
Studies have shown that pulpal health can be compromised at temperature increases of above 5.6°C within the pulp chamber. Alveolar bone necrosis can occur when there is a temperature rise above 7–10°C. The safety threshold for the periodontal ligament is a temperature rise above 10°C for greater than 1 minute.10
Hasegawa et al10 carried out an in vitro study on the effects of radiofrequency-induced heating on a full-arch fixed orthodontic appliance with brackets, molar bands and stainless steel wire and found that the temperature change was +2.61°C. Although this temperature increase would be insufficient to cause damage to the surrounding tissues, the authors postulated that orthodontic appliances may exhibit heating above the European industrial standard (CENELEC standard prEN45502-1) and concluded that the wire should be removed, or a spacer placed between the appliance and the oral mucosa duringMRI.10
Görgülü et al3 evaluated the effects on various combinations of brackets, archwires and ligatures of radiofrequency heating and magnetic interactions during 3-T MRI. They found that none of the groups exhibited excessive heating, with the highest temperature change being <3.04°C. They concluded that the temperature changes were within acceptable ranges and not high enough to affect the pulpal or mucosal health of the oral cavity. However, the authors also noted that nickel–titanium and stainless steel wires caused magnetic interactions that may pose a risk of movement in situ and recommended their removal before MRI.2
A well-known and potentially catastrophic effect of MRI is the mechanical displacement of objects containing ferromagnetic and other magnetic materials. The strong static magnetic field of the scanner can exert an attractive or a torque force on objects within or near the field. This is known as the ‘projectile effect’ and can pose significant risks to patients. There can be movement of ferromagnetic materials, which can cause discomfort of injury to patients.9 Studies have been carried out to evaluate the mechanical displacement effects of fixed orthodontic appliances and have had mixed conclusions. The general consensus however, appears to be that fixed orthodontic components are safe to use in MRI scanners as long as they are securely attached.1,8,11,12
Görgülü et al3 studied the effects of fixed orthodontic appliances on magnetic interactions during 3-T MRI and found that, while the average deflection angle for stainless steel brackets was 13°, the deflection angles for nickel–titanium archwires and stainless steel archwires were 71° and 62°, respectively. A deflection angle of <45° indicates that the deflection force is less than the force of gravity, and that the device does not pose any risk during MRI. The torque force exhibited by the brackets was also found to be mild. Nickel–titanium wire exhibited moderate torque and stainless steel wire exhibited strong torque. The authors concluded that, while brackets do not present a risk during 3-T MRI and can be considered ‘MR safe’, nickel–titanium and stainless steel wires pose a potential risk. They went on to advise that the wires be removed prior to imaging for the patient's safety.2
Zachriat et al5 stated that acceleration and torsion have a negligible impact on attachments that are satisfactorily fixed. The authors cited a study by Sung et al13, who observed forces of 61–104N required for debonding in different bracket materials. They also cited Klocke et al14, who found that a complete orthodontic appliance consisting of stainless steel brackets, ligature wires and arch wires only experienced forces of 1.69N when exposed to a strong 3-T magnetic field.5
Artefact formation
An artefact may be defined as ‘a distortion in MR image signal intensity with no identifiable anatomical source in the imaging field’15 or, more simply, ‘pixels that do not faithfully represent the tissue components under study’.1 Factors that can lead to artefact formation include patient movement, fluid flow and the presence of metallic objects, such as pacemakers, surgical clips, foreign bodies and dental materials.16,17
Metal artefacts occur at the interfaces between soft tissue and soft tissue or ferromagnetic metal, where there are differing magnetic susceptibilities. There is a distortion of the external magnetic field by local magnetic fields that can lead to image distortion and signal loss.17 The size or shape of an image can be distorted, the extent and severity of which being dependent on the metallic object's size, shape, location, orientation, its distance from the anatomical region being imaged, the nature of the alloy, and the MRI sequence and sequence parameters used.1,4,7,11,18,19
Dental alloys are a major source of metal artefacts. Certain metallic components of fixed orthodontic appliances have been shown to produce significant artefacts that can render MRI scans difficult or impossible to interpret.3,20Table 1 summarizes the evidence on the effects of archwires, brackets and bonded retainers on MRI scans.
Proposed protocol
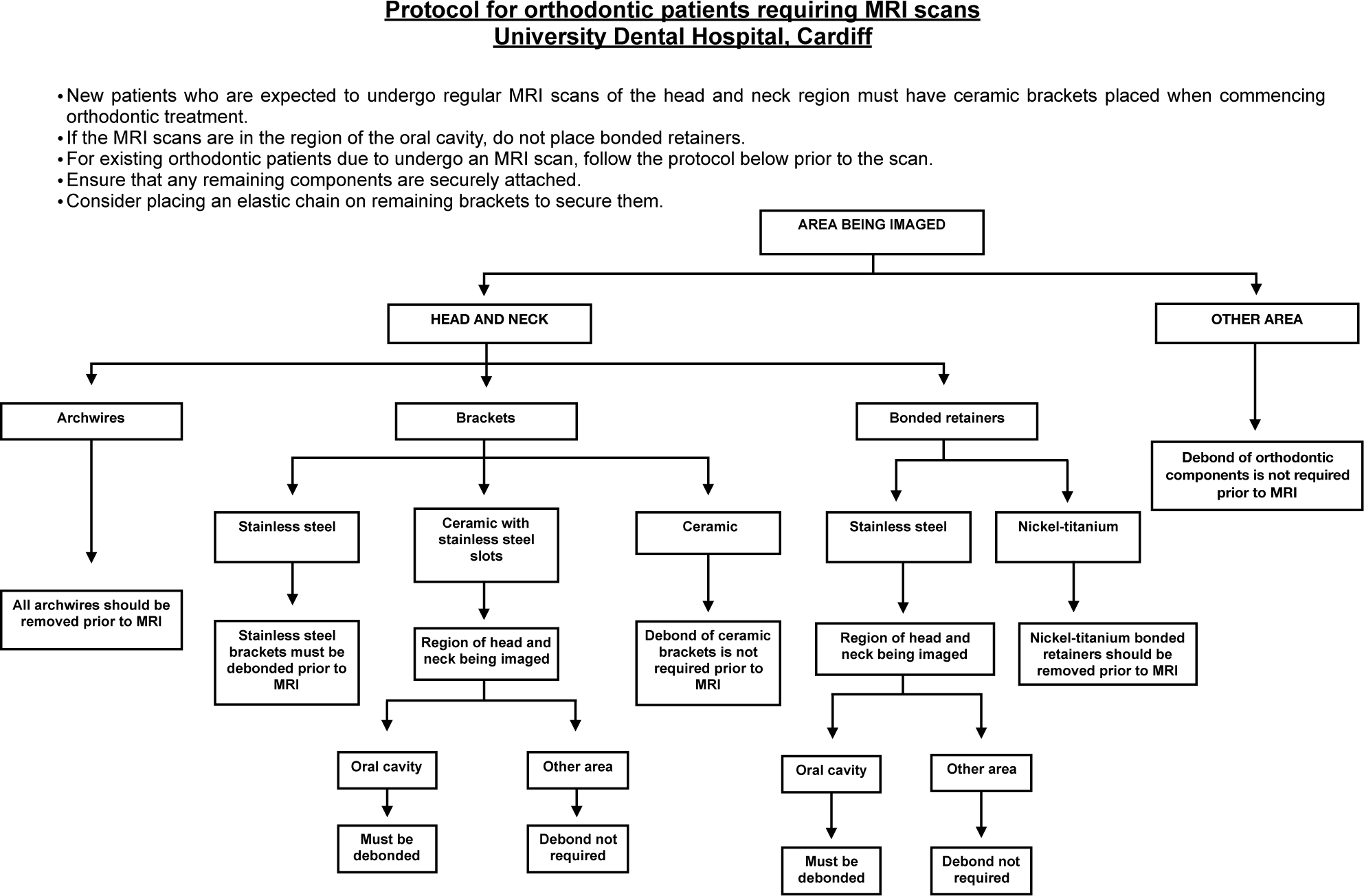
Figure 1 shows the proposed local protocol for the Orthodontics Department at Cardiff Dental Hospital based on the evidence from the literature search. A thorough medical and surgical history should be taken for all new patients to enable early identification of patients who may require MRI scans of the head and neck region during the course of orthodontic treatment. These patients should have ceramic brackets placed as part of their fixed appliance treatment. For existing patients undergoing MRI scans, the protocol should be followed.
Figure 1. Proposed protocol.
Conclusion
As the use of MRI continues to increase and evolve, it is becoming more likely that orthodontists will see patients requiring MRI scans of the head and neck region. It is therefore imperative to understand the unwanted effects that can occur as a result of orthodontic materials being placed in MRI scanners. An evidence-based protocol has been proposed to aid the clinician in the decision-making process about which components should be removed. Further research on the effects of fixed orthodontic appliances on defined anatomical regions of head and neck MR images, and the impact of using different MRI sequences and sequence parameters would be beneficial. More studies of higher scientific quality are required to strengthen the current evidence base, especially regarding artefact formation.