Andreasen JO, Pindborg JJ, Hjorting-Hansen E, Axell T Oral health care: more than caries and periodontal disease. A survey of epidemiological studies on oral disease. Int Dent J. 1986; 36:207-214
Bishara SE Impacted maxillary canines: a review. Am J Orthod Dentofacial Orthop. 1992; 101:159-171
Becker A, Zogakis I, Luchian I, Chaushu S Surgical exposure of impacted canines: open or closed surgery?. Semin Orthod. 2016; 22:27-33
A common way of treating impacted teeth is by orthodontic extrusion. When the teeth are deeply buried in the alveolar bone a closed eruption technique is often indicated. When multiple teeth are impacted and need to be extruded in a particular sequence, it may be difficult to be sure which eruption chain is attached to a particular tooth. This case report demonstrates a novel way of identifying individual eruption chains.
CPD/Clinical Relevance: This case report demonstrates a novel way of identifying individual eruption chains attached to multiple impacted teeth.
Article
Adele Bronkhorst
Dental impaction can be defined as a tooth that is prevented from erupting into position because of a malposition, lack of space or other impediments.1 Although it has been reported to affect as many as 25% to 50% of the population, multiple impactions are less commonly seen.2
According to a review by Bishara, the causes of tooth impaction can be divided into generalized and localized factors.3 The more common localized and generalized factors are summarized in Table 1.
Local Factors
Generalized Factors
Crowding
Past irradiation of the area
The presence of supernumerary teeth
A history of febrile diseases
Prolonged retention or early loss of primary teeth
Certain syndromes, eg cleidocranial dysplasia, Gardner and Down syndromes
The impaction of multiple permanent teeth occurs less frequently than that of single teeth. Multiple impactions add significant complexity to treatment, often resulting in lengthened overall treatment time.
Factors reported to increase treatment complexity and time include:
Age at the start of treatment;
Degree of root formation;
Position and distance of the tooth from the occlusal plane;
Degree of dilacerations.
During treatment there is a further risk of failure due to ankylosis, external root resorption, and/or root exposure during or after orthodontic tooth movement.
When faced with multiple impacted teeth in ectopic positions, it may not be easy to identify which eruption chain is attached to a particular tooth. When a complex case presented with multiple impacted teeth, the team came up with a novel way to identify the chains and which teeth they were connected to.
History, diagnosis and initial treatment plan
A healthy, non-syndromic 9-year-old female patient was referred regarding ‘delayed eruption of the maxillary incisors and the presence of a maxillary midline supernumerary tooth’. A DPT radiograph confirmed the presence of a mesiodens and delayed root maturation of the maxillary incisors (Figure 1). As per the Royal College of Surgeons Guidelines for Management of Unerupted Maxillary Incisors (2010), treatment was provided to remove the primary central incisors and the mesiodens and then monitor permanent incisor eruption.
Figure 1. DPT radiograph exposed (aged 9 years) demonstrating delayed dental age, presence of midline supernumerary tooth and unerupted maxillary central incisors.
Treatment progress and treatment plan review
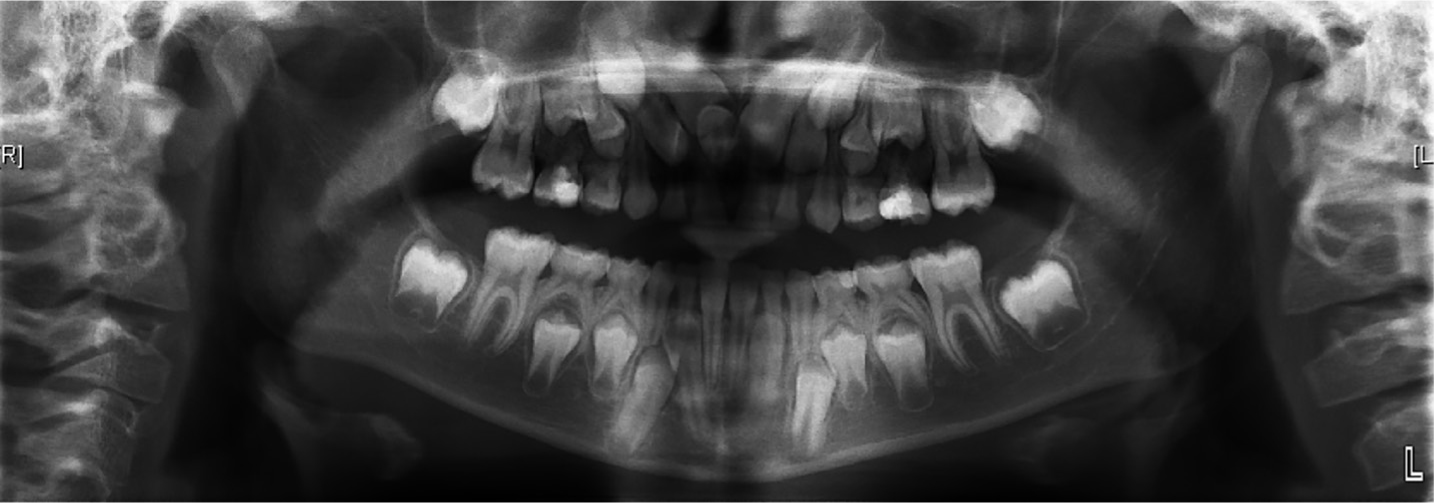
Eruption was monitored following the extractions. The patient was again clinically reviewed by both the orthodontist and the surgeon at age 11 years. Her overall dental development was still delayed. The UL1 had partially erupted into the dental arch. However, the UR4, UR3, UR2, UR1, UL2, UL3 were still unerupted and in unfavourable positions (Figure 2).
Figure 2. DPT radiograph exposed (aged 11 years) following extraction of the supernumerary tooth demonstrating delayed dental age, presence of unerupted maxillary incisors.
Due to the position of the unerupted permanent incisors and canines and lack of improvement, it seemed unclear if these teeth were likely to improve spontaneously. The patient's family were keen to try to align the teeth without extraction of adult teeth.
After careful consideration, active intervention was proposed including extraction of URC, URB, ULB and ULC. The closed eruption technique with gold chain bonded on the UR4, UR3, UR2, UR1, UL1, UL2, UL3 was planned to aid orthodontic extrusion of these teeth. A modified Nance transpalatal arch was proposed to transfer the extrusive force onto the teeth via the eruption chains.
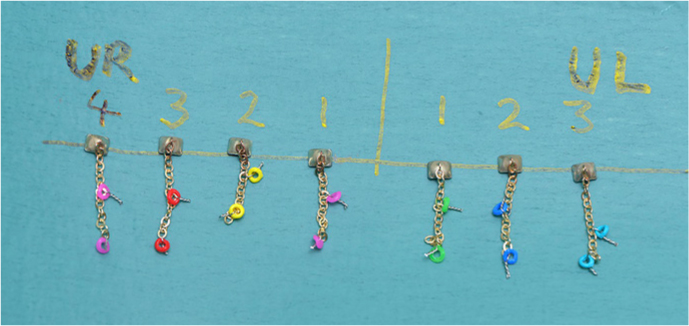
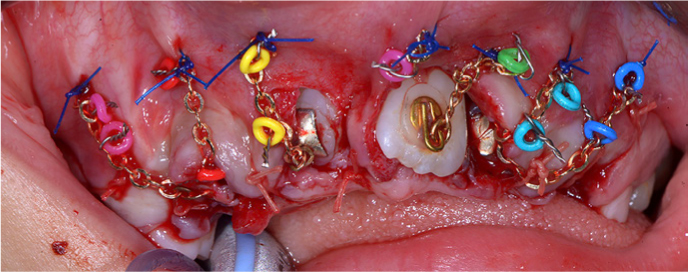
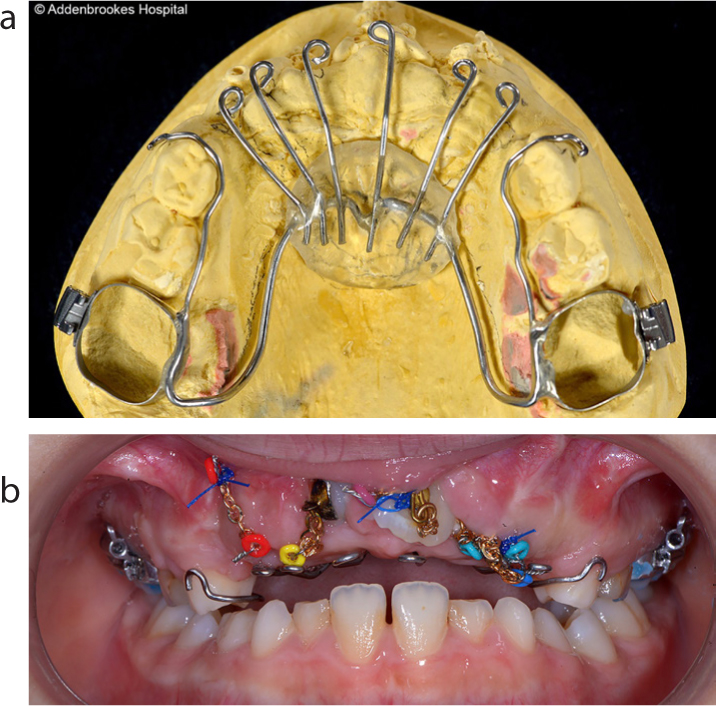
Prior to surgery, the gold chains were colour coded by attaching two similarly coloured elastic modules (3M Unitek) to each gold chain with 0.010” SS ligature wire (Figure 3). Once visualized following adequate bone removal, a predetermined colour coded gold chain was attached to each exposed tooth. Prior to flap closure, bond strength was tested. The gold chains were passed transmucosally and the flaps were sutured into position. The chains were ligated with 3/0 prolene sutures to the gingival tissues. No eruptive force was placed on the day of exposure (Figure 4). Three weeks later a modified Nance transpalatal arch was placed (Figures 5a and b) and extrusive force applied.
Figure 3. Colour coding of chains according to tooth number.Figure 4. Chains sutured onto the gingival tissues following exposure.Figure 5.
(a) Modified Nance transpalatal bar. (b) Intra-oral view of Nance transpalatal bar in situ with chains attached.
Discussion
Patients with multiple impactions need co-ordinated, multidisciplinary management to guide eruption of as many teeth as possible. It is important to set realistic treatment goals and teeth that cannot successfully be brought into the arch may require extraction followed by either space closure or prosthetic replacement.
The timing of orthodontic treatment, type of surgery to uncover the impacted tooth, orthodontic mechanics necessary and potential problems vary according to which tooth/teeth are impacted.
The aim of surgical uncovering is:
To eliminate any hard or soft tissue pathology/obstructive entities;
To provide the orthodontist with access to the impacted tooth usually by creating a suitable area to bond an attachment to;
Minimal tissue damage to adjacent structures and the cemento-enamel junction and root of the impacted tooth/teeth to be exposed.4
The wide mucosal flap employed in the closed eruption technique allows for better vision and haemostasis (thus implied improved bonding) and increases the range of impacted teeth that can be salvaged.
This case presented with impacted teeth and crowns in close proximity to one another. These teeth needed to be extruded in a particular sequence, with particular force vectors. Therefore it was vital to be able to identify which chain is attached to a specific tooth to enable predictable eruptive mechanics.
The crowns of UL2 and UL3 were positioned in a similar AP plane and the chains entered the oral cavity in virtually the same position. This could have led to confusion as to which chain to apply traction. By identifying the dark blue marked chain, it was possible to apply extrusive force to the UL2 with confidence. When attaching the light blue chain of the UL3 to the modified Nance appliance, it was easy to identify that this is the chain that required a distal component of force. As the teeth erupt, the force vectors and eruption sequence may need to be adapted and it will remain a predictable task to identify which chain is attached to which impacted tooth.
Conclusion
The technique devised is a novel, cost-effective way to identify different eruption chains, allowing the orthodontist to apply force vectors confidently, as required in complicated cases with multiple impacted teeth. This technique can be easily adapted into clinical practice to deliver targeted, predictable traction to unerupted teeth.