Negi A, Negi A, Mohanan M Solitary median maxillary central incisor syndrome: a rare entity. J Oral Maxillofac Pathol. 2020; 24 https://doi.org/10.4103/jomfp.JOMFP_183_19
Kjaer I, Becktor KB, Lisson J Face, palate, and craniofacial morphology in patients with a solitary median maxillary central incisor. Eur J Orthod. 2001; 23:63-73 https://doi.org/10.1093/ejo/23.1.63
Dolan LM, Willson K, Wilson WG 18p-syndrome with a single central maxillary incisor. J Med Genet. 1981; 18:396-368 https://doi.org/10.1136/jmg.18.5.396
Masuno M, Fukushima Y, Sugio Y Two unrelated cases of single maxillary central incisor with 7q terminal deletion. Jinrui Idengaku Zasshi. 1990; 35:311-317 https://doi.org/10.1007/BF01883753
Tekendo-Ngongang C, Muenke M, Kruszka P Holoprosencephaly overview. (updated 2020). In: Adam MP, Feldman J, Mirzaa GM (eds). Seattle, WA, USA: University of Washington;
Lukez A, Pavlic A, Trinajstic Zrinski M, Spalj S The unique contribution of elements of smile aesthetics to psychosocial well-being. J Oral Rehabil. 2015; 42:275-281 https://doi.org/10.1111/joor.12250
Hughes S, Balmer R, Moffat M, Willcoxson F The dental management of children with congenital heart disease following the publication of Paediatric Congenital Heart Disease Standards and Specifications. Br Dent J. 2019; 226:447-452 https://doi.org/10.1038/s41415-019-0094-0
Scottish Dental Clinical Effectiveness Programme. Antibiotic prophylaxis. Implementation advice for national institute for health and care excellence (nice) clinical guideline 64 prophylaxis against infective endocarditis. 2018. http//www.sdcep.org.uk/published-guidance/antibiotic-prophylaxis/ (accessed March 2024)
National Institute for Clinical Excellence. Prophylaxis against infective endocarditis: antimicrobial prophylaxis against infective endocarditis in adults and children undergoing interventional procedures. 2016. http//www.nice.org.uk/guidance/cg64 (accessed March 2024)
Riveros Gilardi B, Munoz Lopez JI, Hernandez Villegas AC Types of cerebral herniation and their imaging features. Radiographics. 2019; 39:1598-1610 https://doi.org/10.1148/rg.2019190018
Karolyhazy K, Kivovics P, Fejerdy P, Aranyi Z Prosthodontic status and recommended care of patients with epilepsy. J Prosthet Dent. 2005; 93:177-182 https://doi.org/10.1016/j.prosdent.2004.11.008
Harrison M, Calvert ML, Longhurst P Solitary maxillary central incisor as a new finding in CHARGE association: a report of two cases. Int J Paediatr Dent. 1997; 7:185-189 https://doi.org/10.1046/j.1365-263x.1997.00236.x
Sajnani AK, King NM Dental anomalies associated with buccally and palatally impacted maxillary canines. J Investig Clin Dent. 2014; 5:208-213 https://doi.org/10.1111/jicd.12035
Ericson S, Kurol PJ Resorption of incisors after ectopic eruption of maxillary canines: a CT study. Angle Orthod. 2000; 70:415-423
Ericson S, Kurol J Incisor root resorptions due to ectopic maxillary canines imaged by computerized tomography: a comparative study in extracted teeth. Angle Orthod. 2000; 70:276-283
A multidisciplinary approach to managing a missing central incisor, impacted canines and complex medical history: a case report Judi Humphreys Asma Keshtgar Cathy Bryant Maalini Patel Sanjeev Sood Shruti Patel Dental Update 2024 17:2, 707-709.
Hypodontia of a maxillary central incisor is infrequent and can indicate Solitary median maxillary central incisor syndrome. We report on an 11-year-old child with medical comorbidities who presented with hypodontia of a maxillary central incisor, buccally impacted maxillary canines and root resorption of the maxillary lateral incisors. She had previously had dental extractions. Joint orthodontic–paediatric–oral surgery treatment included loss of the maxillary lateral incisors and fixed orthodontic appliances to idealize space for prosthetic replacement of a central incisor. The value of multidisciplinary planning is emphasized and the dental considerations for patients with complex medical histories explored.
CPD/Clinical Relevance: The reader should have an understanding of the importance of a joint orthodontic-paediatric-oral surgery approach when managing complex paediatric dental patients.
Article
Solitary median maxillary central incisor (SMMCI) syndrome is a rare genetic condition that affects approximately 1:50,000 live births.1 It is characterized by hypodontia of a central incisor, with the remaining incisor appearing symmetrical, and is often associated with multisystem defects usually in the midline of the body.1 Structural defects may include absence of the upper labial frenum, an unclear philtrum, nasal cavity anomalies, septal deviation, ridge down midline of palate and hypotelorism.2 While the exact pathophysiology is not well understood, it has been reported that defects in the sonic hedgehog gene and deletion of parts of chromosome 18 and 7q can result in SMMCI syndrome.2,3,4 Genetic testing may be appropriate because it often presents as part of the phenotypic spectrum of holoprosencephaly. Holoprosencephaly occurs when the prosencephalon (embryonic forebrain) fails to divide into two separate lobes. It can also result in microcephaly, hypotelorism, single maxillary incisors and cleft lip and palate. It varies in severity with the condition being fatal prior to birth for some children, and others having nearly normal brain development.5,6 A multidisciplinary approach to the management of patients who present with one or more signs of SMMCI is therefore recommended.
Smile aesthetics and the underlying malocclusion are significant contributors to psychological wellbeing.7 Treatment planning for the replacement of a missing maxillary central incisor should, therefore, be made at the earliest possible stage with considerations regarding the amount of space required for the replacement maxillary incisor and a clear appreciation of the need to plan carefully its immediate, intermediate, and long-term restorative replacement. In some patients, it will be possible to mesialize a maxillary lateral incisor tooth and mask this as a maxillary central incisor; however, this is very case dependent with many factors, including gingival margin morphology, the underlying malocclusion and patient/family wishes, all playing a significant role in case selection. The long-term restorative burden of any treatment provided should not be overlooked, and the patient/family should appreciate the commitment required.
Clinical case
The patient was referred to the orthodontic department from specialist orthodontic practice for the surgical removal of her impacted UR3 and UL3 at the age of 11 years.
The patient presented with a complex medical history (Table 1). At the age of 9 months, she underwent successful surgical correction for tetralogy of Fallot. At 3 years old, she was diagnosed with cerebellar herniation through the foramen magnum, although she remains asymptomatic. Fusion of some cervical vertebrae and cerebellar herniation presented a potential contraindication to neck extension during general anaesthetic, but after confirmation that it was safe to extend her neck during the procedure her tonsils were removed to address symptoms of sleep apnoea. In addition, she also has epilepsy, Duane syndrome affecting adduction and abduction of the eye, and hearing loss.
Table 1. The patient's medical history
Fully repaired tetralogy of Fallot
Cerebellar tonsil herniation
Fusion of cervical vertebrae
Spinal kyphoscoliosis
Tonsillar hypertrophy
Epilepsy
Duane syndrome
Hearing loss
Congenital mirror movement of hands
Clinical findings
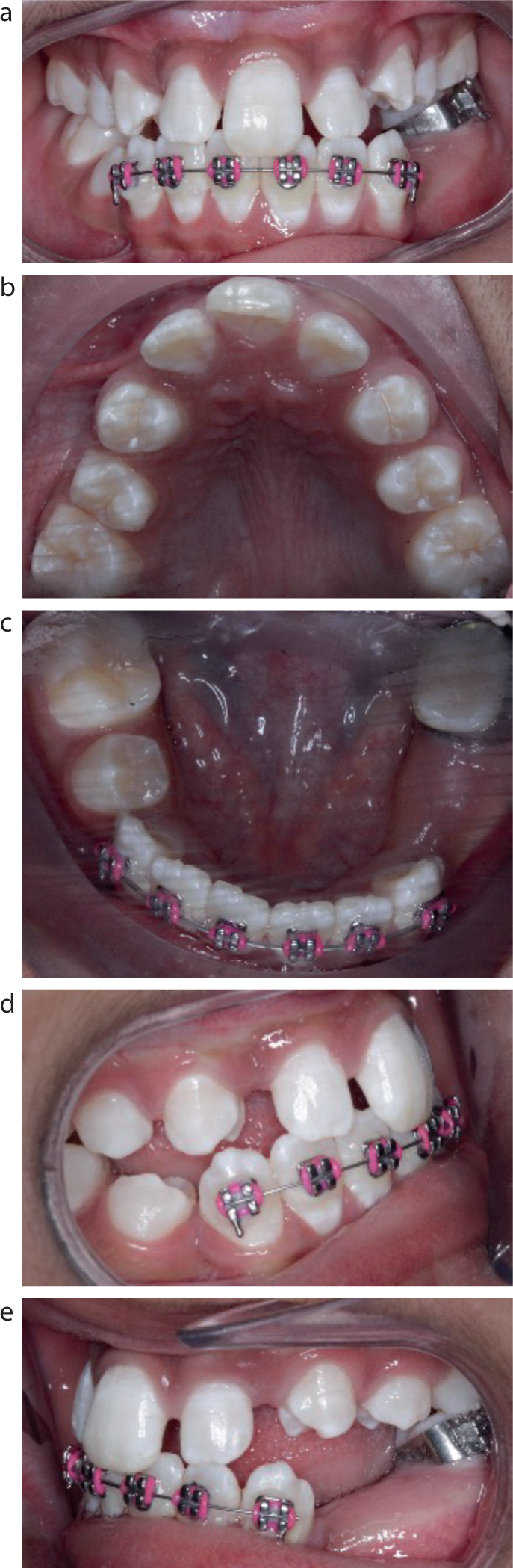
The patient was in the permanent dentition with a Class III incisor relationship on a mild skeletal 3 base. Her malocclusion was complicated by hypodontia of an upper central incisor, buccally impacted maxillary permanent canines and root resorption of the maxillary permanent lateral incisors. The lower first premolars had been extracted and the lower left second premolar was unerupted. The maxillary arch was V-shaped and the lower arch U-shaped. The maxillary central incisor was located in the midline and previous genetic investigation had not identified a cause for this.
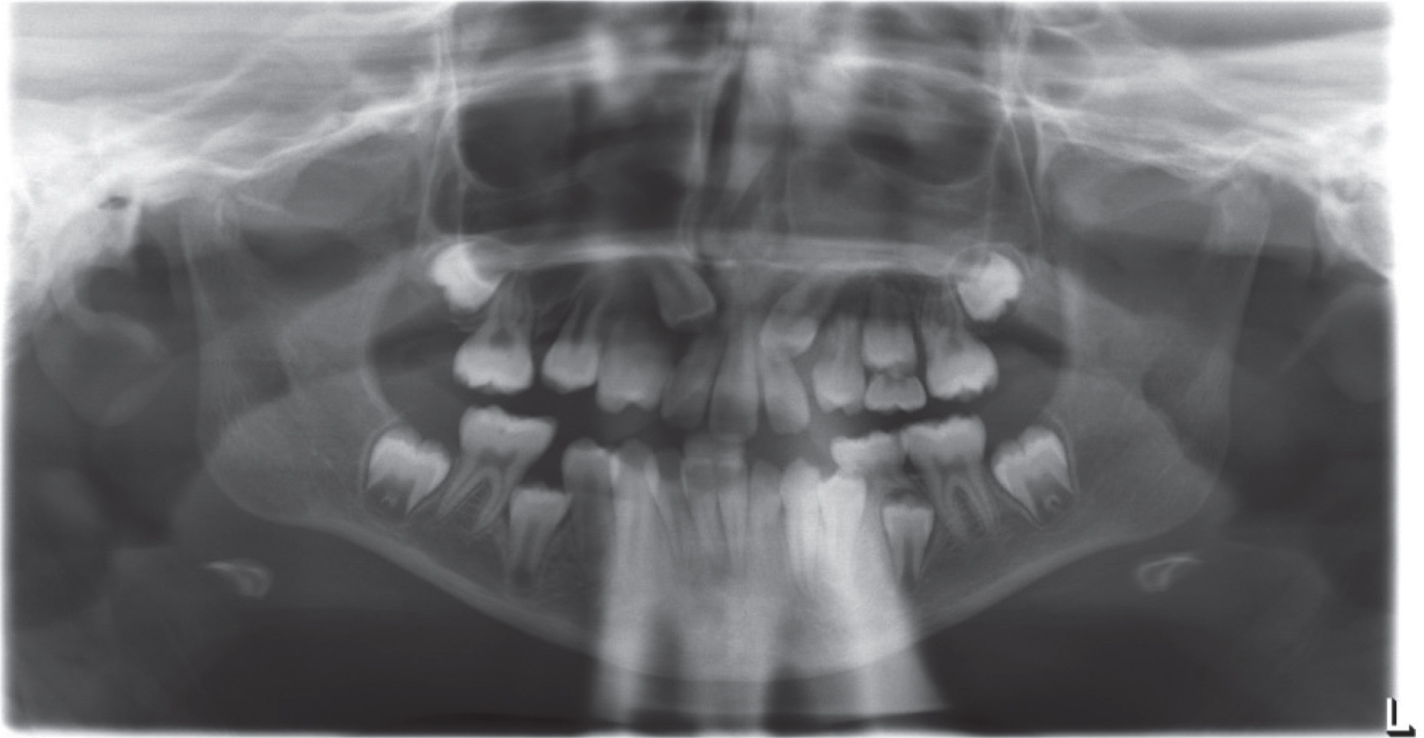
On attendance, she presented with a lower sectional fixed orthodontic appliance extending from LR3 to LL3, which had been placed in specialist orthodontic practice and had been in situ for approximately 3 months (Figures 1 and 2).
Figure 1. (a–e) Intra-oral photographs at the initial presentation.Figure 2. Pre-treatment orthopantogram sent with referral
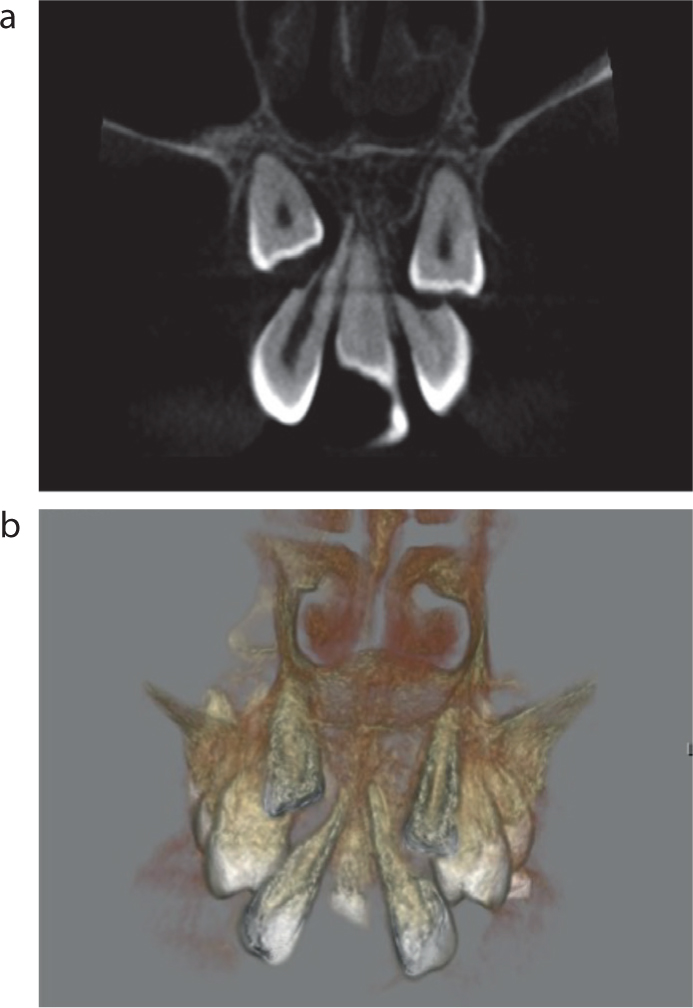
CBCT imaging was used to investigate potential resorption to the lateral incisors. It showed that the impacted maxillary permanent canines had caused severe resorption of the lateral incisors (Figure 3).
Figure 3. (a,b) CBCT imaging demonstrating extensive resorption of UR2 and UL2.
Treatment planning
Based on her presenting malocclusion, medical history and patient/family wishes, the following treatment plan was devised:
Extraction of UR2 and UL2 under local anaesthetic supplemented with inhalation sedation and then await eruption of UR3 and UL3;
Upper removable appliance (URA) for expansion and pontics to replace UR2 and UL2 prior to the canines erupting;
Upper and lower fixed orthodontic appliances to align the dentition and idealize space for future prosthetic replacement of UR1;
Long-term retention.
The alternative treatment option was surgical extraction of the impacted UR3 and UL3, followed by upper and lower fixed orthodontic appliances to idealize space for future prosthetic replacement of the UR1. Long-term retention would also be required. While this alternative treatment option would have reduced the orthodontic treatment duration, this was not the preferred option as the upper lateral incisors, which had a poor prognosis owing to the significant root resorption, would be retained and a general anaesthetic would be required for the surgical extractions.
Treatment
The maxillary lateral incisors were successfully removed under inhalation sedation, and an upper removable appliance was fitted to allow maxillary arch expansion while restoring anterior spaces for aesthetics and space maintenance.
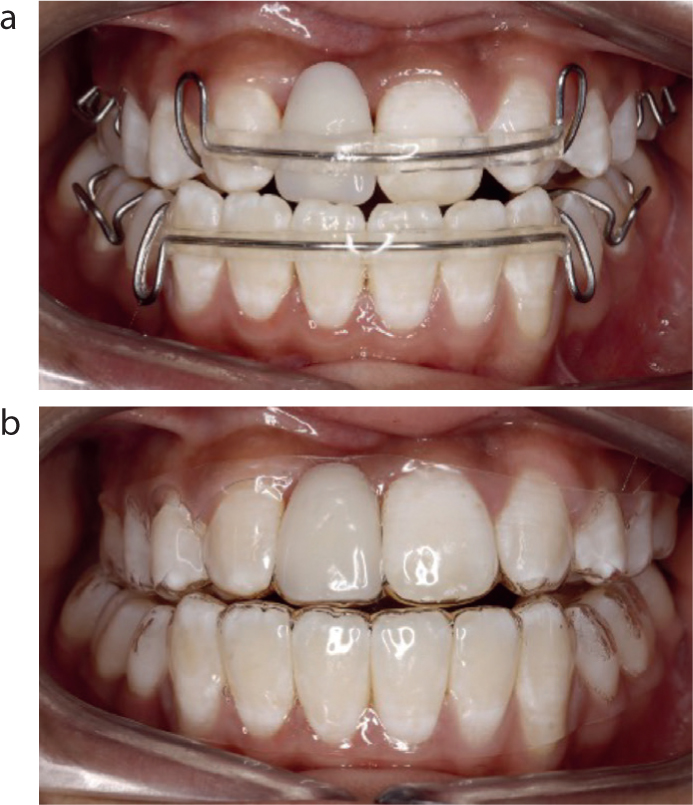
Following expansion, a fixed labial appliance was then placed from UR5 to UL5 while the UR3 remained unerupted. At following visits, the UR6, UR3 and UL6 were bonded and a push coil was placed to move the UL1 distally. Once enough space was present, a pontic to replace the UR1 was provided (Figure 4). At this time, it was noted that the incisor relationship was becoming more Class III. The patient opted to have her lower arch aligned, although she was made aware that a reverse overjet would have to be accepted. As marked shortening of her premolar roots was noted radiographically at 18 months into treatment (Figure 5), debond was planned at this stage. A resin-bonded bridge was fitted following this to replace the UR1 (Figures 6–8).
Figure 4. (a,b) Hawley and vacuum-formed retainers with UR1 pontic.Figure 5. Orthopantomogram demonstrating generalized shortening of roots.Figure 6. Final result with resin bonded bridge.Figure 7. (a–d) Extra-oral photographs of patient at retainer review appointment.Figure 8. (a–d) Intra-oral photographs of patient at retainer review appointment.
Discussion
This patient's care was challenging to manage owing to her complex medical history, and multiple dental anomalies. Treatment was delayed during the COVID-19 pandemic because the patient was advised to shield for a prolonged period: she was considered to be clinically vulnerable owing to her medical history.
Tetralogy of Fallot accounts for 5–10% of congenital cardiac defects (CCD) with an incidence of 5–9 per 1000 births.8 It consists of four defects: ventricular septal defect; pulmonary stenosis; overriding aorta; and right ventricular hypertrophy. It is considered a cyanotic CCD owing to the flow of deoxygenated blood from right to left ventricles, which mixes with oxygenated blood from the lungs, decreasing the total oxygen levels in the circulating blood.9 The patient had successful cardiac surgery before her first birthday, meaning she experienced no restriction to her activity levels and required no cardiac medications. As the cardiac defect had been fully repaired, with only trivial turbulence of blood flow through valves, her risk of developing infective endocarditis was lowered and her cardiac team did not recommend the use of antibiotic prophylaxis prior to dental treatment.10,11
Further potential risks related to the presence of several fused cervical vertebrae, which may have restricted the extension of her neck during dental procedures under general anaesthetic. In addition, she was found to have cerebellar herniation through the foramen magnum, which can result in life-threatening complications.12 These findings were investigated thoroughly by her paediatric neurology team, who advised she was not at risk of damage to her neck or pressure to her brain stem in extension or flexion. Positioning during general anaesthetic or dental procedures were therefore deemed safe.
The patient also experienced epilepsy. Generally, a fixed prosthesis is preferred in patients with epilepsy to avoid inhalation/choking if a removable prothesis were to become loose or fracture during a seizure.13 However, as her epilepsy was well controlled, use of an upper removable appliance and removable retainer were considered appropriate in this case.
SMMCI has been associated with other conditions and syndromes including holoprosencephaly,6 Duane syndrome, CHARGE syndrome, VACTERL association, DiGeorge syndrome, Goldenhar syndrome, and ectodermal dysplasia.1,14 The patient shared some of the features of two of these syndromes. The stigmata of CHARGE syndrome include deafness and cardiac defects,15 while those of VACTERL association16 include vertebral abnormalities, such as scoliosis, cardiac abnormalities and limb anomalies. The patient had genetic testing as a child, but none of the discussed conditions were identified. She does, however, have a formal diagnosis of Duane syndrome.
The complexity of the patient's medical history alone would suggest multidisciplinary, hospital-based dental care would best meet her needs, in addition to multiple dental anomalies. Starting orthodontic treatment in specialist practice before multidisciplinary planning resulted in unnecessary prolongation of orthodontic treatment. A decision for early cessation of fixed orthodontic treatment was made as significant root shortening was noted.
The patient presented with multiple anomalies, including SMMCI and bilateral impacted canines, which had caused severe resorption to the lateral incisors. She was therefore left with only one viable maxillary incisor, which worsened her Class III tendency. Several publications have investigated the occurrence of multiple dental anomalies in the same patient, and this can further complicate management. Sajnani et al found that almost half of patients (47.5%) presenting with ectopic canines exhibited another dental anomaly.17 In patients who are found to have a dental anomaly, careful clinical and radiographic assessment should be undertaken in order for any further anomalies to be identified.
CBCT is a more sensitive tool for diagnosing resorption than conventional two-dimensional imaging; this was the indication for its use in this case.18,19 Confirmation of significant resorption of the maxillary lateral incisors had an important bearing on the treatment planning since the original referral was for surgical removal of the maxillary permanent canines, leaving the lateral incisors in situ. If the maxillary canines had been extracted, the patient would have been left with two poor-prognosis lateral incisor teeth that would eventually require replacement, with no canine teeth to use as abutments. With three missing teeth in the maxillary incisor area and a Class III skeletal base, it was not feasible to camouflage the incisor relationship. The patient and her family were happy to accept a Class III incisor relationship. Orthognathic surgery was not considered given that the patient had no facial or functional concerns, the Class III skeletal pattern was not severe and root shortening was displayed. A long treatment plan may have caused further root damage and, given the patient's medical complexity, elective surgery would be best avoided.
Fortunately, the patient was able to tolerate extraction of the UR2 and UL2 under local anaesthetic and inhalation sedation, thus the use of general anaesthesia was unnecessary. It is generally accepted as good practice to minimize the number of general anaesthetics that a patient undergoes, to reduce the risk of harm to them. Had the patient required extractions under general anaesthetic, attempts to combine the ENT and paediatric dentistry procedures required would have been made.
Conclusion
Multidisciplinary planning with input from consultants in paediatric dentistry, orthodontics, and oral surgery with experience in managing complex cases was key to managing the intricacies of this case, diagnosing all anomalies and pathology. This ultimately led to an excellent outcome that met the patient's needs.
The extraction of poor-prognosis teeth should be considered early as part of a holistic treatment plan to reduce the long-term dental burden for the patient.
A full history, examination and investigation should be undertaken for patients with hypodontia of a central incisor because this may be suggestive of solitary median maxillary central incisor syndrome.