Geron S, Shpack N, Kandos S, Davidovitch M, Vardimon AD. Anchorage loss – a multifactorial response. Angle Orthod. 2003; 73:730-737
Klontz H. Tweed-Merrifield sequential directional force treatment. Semin Orthod. 1996; 2:254-267
Root TL. The level anchorage system for correction of orthodontic malocclusions. Am J Orthod. 1981; 80:395-410
Melsen B, Verna C. A rational approach to orthodontic anchorage. Prog Orthod. 1999; 1:10-22
Chung K, Nelson G, Kim S, Kook Y. Severe bidentoalveolar protrusion treated with orthodontic microimplant-dependent en-masse retraction. Am J Orthod Dentofacial Orthop. 2007; 132:105-115
Block MS, Hoffman DR. A new device for absolute anchorage for orthodontics. Am J Orthod Dentofacial Orthop. 1995; 107:251-258
Umemori M, Suguwara J, Mitani H, Nagasaka H, Kawamura H. Skeletal anchorage system for open bite correction. Am J Orthod Orthop Dentofacial Orthop. 1999; 115:166-174
Chung KR, Kim YS, Linton JL, Lee YJ. The miniplate with tube for skeletal anchorage. J Clin Orthod. 2002; 36:407-412
Kanomi R. Mini-implant for orthodontic anchorage. J Clin Orthod. 1997; 31:763-767
Kyung HM, Park HS, Bae SM, Sung JH, Kim IB. Development of orthodontic micro-implants for intraoral anchorage. J Clin Orthod. 2003; 37:321-328
Park HS, Bae HS, Kyung HM, Sung HM. Micro-implants anchorage for the treatment of skeletal class I bialveolar protrusion. J Clin Orthod. 2001; 35:417-422
Maino BG, Bender J, Pagin P, Mura P. The spider screw for skeletal anchorage. J Clin Orthod. 2003; 37:90-97
Chung KR, Kim SH, Kook YA. C-orthodontic space micro-implant as a unique skeletal anchorage. J Clin Orthod. 2004; 38:478-486
Chung KR, Kim SH, Kook YA. Severe bidentoalveolar protrusion treated with orthodontic micro-implants dependent en-masse retraction. Am J Orthod Dentofacial Orthop. 2007; 132:105-115
Severe bimaxillary dento-alveolar proclination with hyperdivergent jaw bases treated with temporary anchorage devices: a case report Narayan H Gandedkar Ameet V Revankar Orthodontic Update 2025 6:3, 86-91.
Authors
Narayan HGandedkar
BDS, MDS
Clinical and Research Fellow, Department of Craniofacial Dentistry and Orthodontics, Chang Gung Memorial Hospital, Tun Hwa North Road, Taipei, Taiwan and Assistant Professor, Department of Orthodontics and Dentofacial Orthopaedics, SDM College of Dental Sciences and Hospital, Sattur, Dharwad, Karnataka, India
The article describes the orthodontic treatment of a 19-year-old female with severe bimaxillary dento-alveolar proclination and severely hyperdivergent jaw bases. Clinical and cephalometric analyses denoted it to be a critical anchorage case. Accordingly, with the aim of providing absolute anchorage, temporary anchorage devices (TADs) were placed in all four quadrants in the inter-radicular area of the second premolar and first molar, following extraction of all first premolars. Facial aesthetics improved considerably, fullness of the upper and lower lip reduced and incompetency of the lips was eliminated. The application of TADs not only reduced the antero-posterior discrepancy, but also addressed the vertical problem.
Clinical Relevance: The treatment of critical anchorage, hyperdivergent cases with conventional orthodontics has always remained a challenge, with a greater chance of an unsatisfactory treatment outcome. The use of TADs has changed the scenario with the concept of absolute anchorage coming closer to reality.
Article
Narayan Gandedkar Ameet Revankar
Conservation of anchorage is a decisive constituent of en masse retraction.1 Utmost importance is placed on Newton's third law – the law of action and reaction. Orthodontists are sentient of the fact that, for any force applied on the teeth, there will be an equal and opposite reaction.2,3,4 Poor patient compliance can only skew the ‘vector equation’ towards greater anchorage loss and hence unsatisfactory treatment results; these factors have led to the greater exercise of intra-osseous anchorage.5 Use of implants have become more practical as far as conservation of anchorage is concerned.6,7,8,9,10,11,12,13 The mechanics of force application can be simple or complicated, depending on the level of anchorage control necessary. The use of TADs reduces the number of teeth requiring bands or brackets, especially second molars, hence reducing the risk of damage to the periodontium or enamel surfaces.14
Diagnosis
A 19-year-old female attended the orthodontic clinic complaining of forwardly placed upper and lower front teeth, spacing in between the upper front two teeth and difficulty in lip closure. Her medical history was non-relevant and temporomandibular joint function was normal.
Extra-oral examination revealed a convex profile, incompetent lips with reduced philtrum length and increased lower anterior face height. On smiling, the patient exhibited a consonant smile arc (Figure 1). In Sarver's classification of smile lines, this means that the lower lip vermilion border follows the incisal edges of the upper teeth in a frontal smile.
Intra-oral examination showed a bilateral Angle's Class I molar and canine relationship with a midline diastema in the upper arch and moderate crowding in the lower arch with a 90° rotation of the lower left second premolar. The overjet and overbite measured 1.2 mm and 2 mm, respectively. The skeletal midline matched the dental midline (Figure 2).
The patient was diagnosed as Angle's Class I malocclusion with severe bimaxillary dento-alveolar proclination and severely hyperdivergent jaw bases.
Rationale for treatment plan
Taking into consideration the convex profile and the severe space discrepancy in the upper and lower arches, an extraction treatment protocol was followed along with placement of TADs in all the quadrants for conservation of anchorage.
Treatment objectives
In the maxillary and mandibular arches, to obtain space by extraction of all first premolars and utilize for en masse retraction of the anterior segment and for decrowding the lower anterior segment;
Obtaining correct overjet and overbite;
Correction of the convex facial profile to rather straighter;
Eliminating the lip strain along with attainment of the proper lip balance;
Achieve a stable, functional occlusion with a pleasing smile.
Treatment alternatives
Extraction of all four first premolars and use of high pull headgear with TransPalatal Arch (TPA). High pull headgear is used for two reasons. First, to conserve anchorage, secondly to attain vertical control, as the patient has hyperdivergent jaw bases. However, the patient was reluctant to use the headgear.
A surgical line of treatment was also formulated, consisting of a bimaxillary dento-alveolar setback with advancement genioplasty to address the bimaxillary dento-alveolar proclination and recessive chin, respectively, after appropriate orthodontic decompensation. The patient was not enthusiastic about this line of treatment.
The third treatment plan would be to extract all first premolars and the use of TADs placed in the inter-radicular area between the second premolar and first molar in all the four quadrants. The use of TADs will not only conserve anchorage but will also assist vertical molar control.
Treatment progress
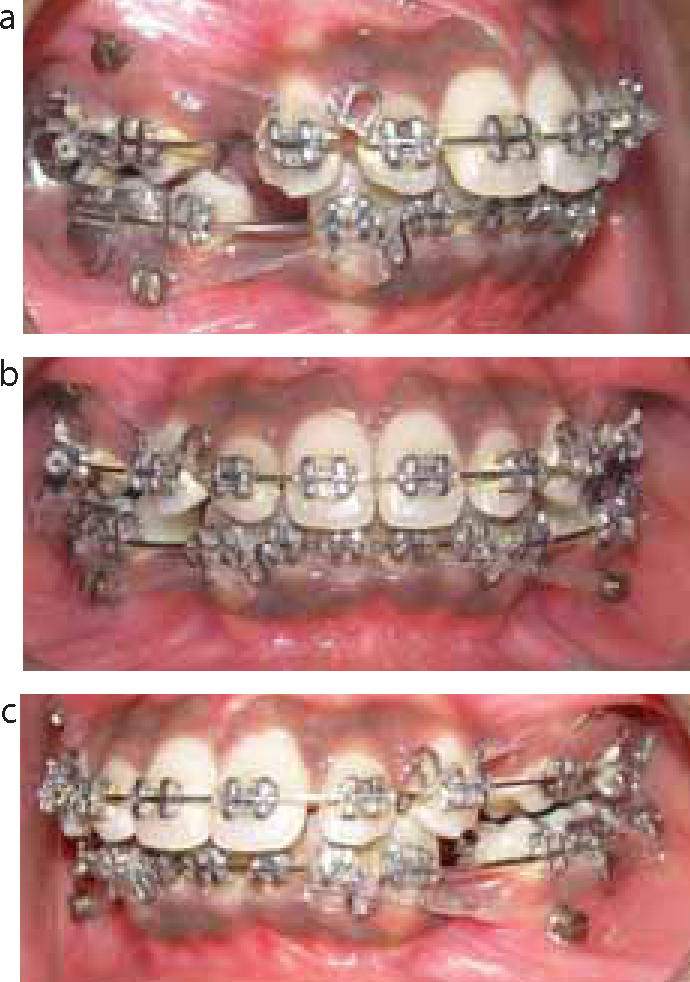
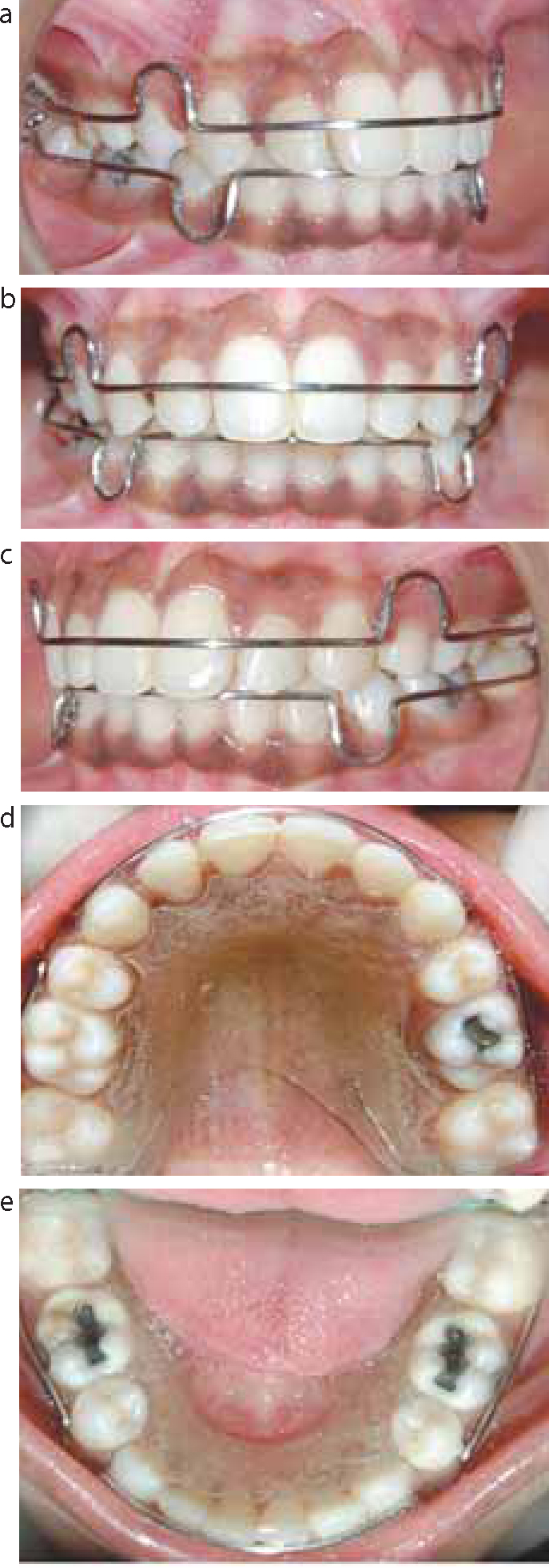
After the formal consent of the patient was obtained, all first premolars were extracted under local anaesthesia. The first molars were banded and the remaining teeth were bonded with a 0.022” Pre-Adjusted Edgewise Appliance (MBT prescription, 3M Unitek, Monrovia, California, USA). Initial levelling in both arches was accomplished with 0.016” NiTi (Orthoforce G4-Nickel Titanium G&H Wire Company, Hanover, Germany) archwires. The severely rotated lower left second premolar was addressed individually by placement of a couple force to correct the rotation. As soon as the rotation was corrected, 0.018” SS wires were placed in the upper and lower arches. No active retraction was undertaken during the levelling and aligning stage. Once levelling and aligning was achieved, however, 0.021” x.025” SS wires were placed in the upper and lower arches with cuspid hooks. TADs, 1.2 x 8 mm in dimension (SK Surgicals®, Pune, India), were placed in the inter-radicular area of second premolar and first molars in all the four quadrants under a topical anaesthetic (Figure 5). Implants were loaded immediately without a waiting period. Using power chains, approximately 200 gm of force was applied, running from the hooks on the continuous archwires to the head of the implant. After seven months of active en masse retraction, settling of the occlusion was completed using 0.016” SS archwires in the upper and lower arches, with settling elastics, for a period of three months. Some space was maintained mesial to the upper right canine as the upper right lateral incisor was smaller in size than the norm. After debonding the appliance, the lateral incisor was built up with hybrid Bis-GMA composite resin to match the contralateral lateral incisor.
Figure 5.
(a–c) TADs placed in the inter-radicular area of first molar and second premolar in all the quadrants.
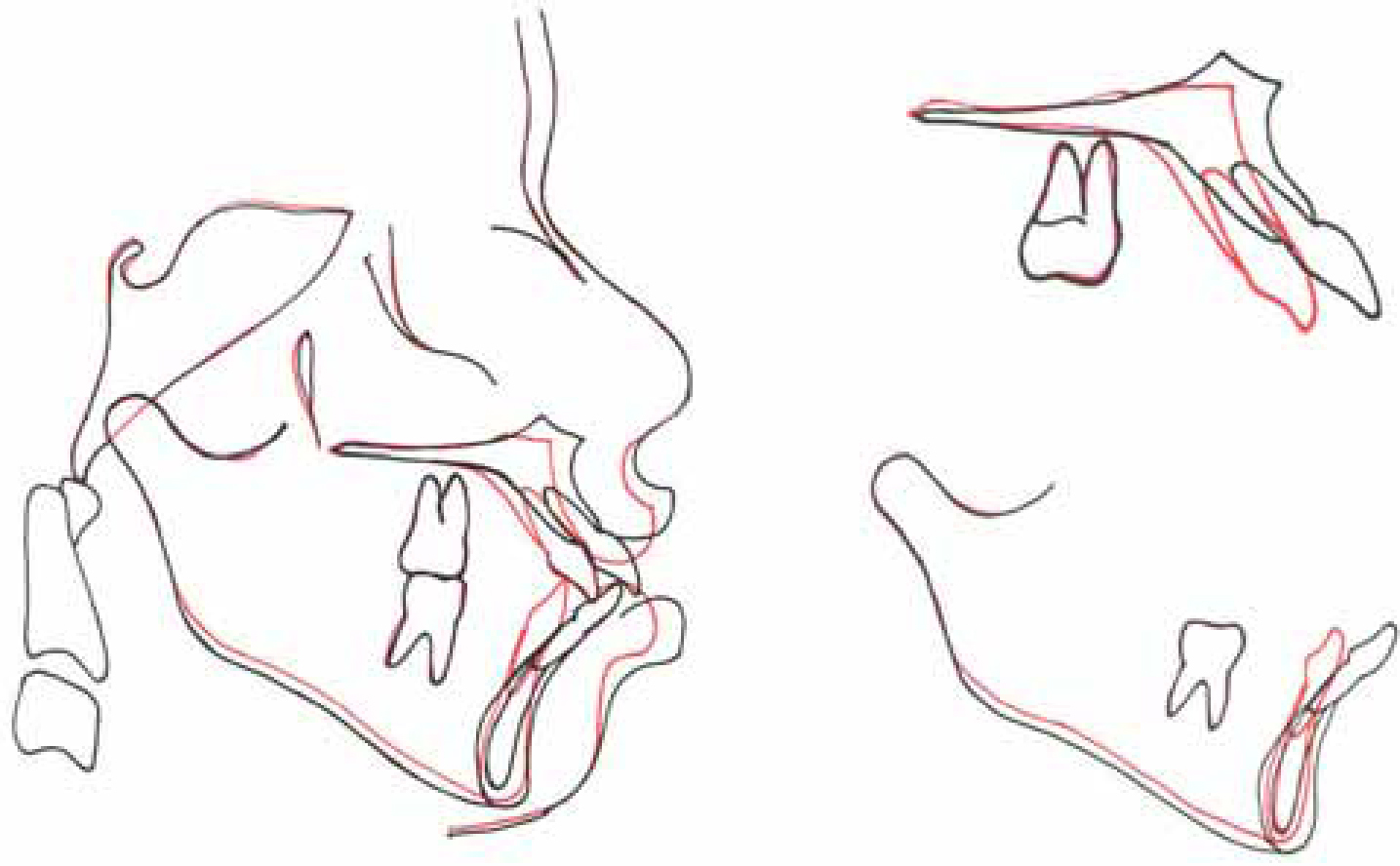
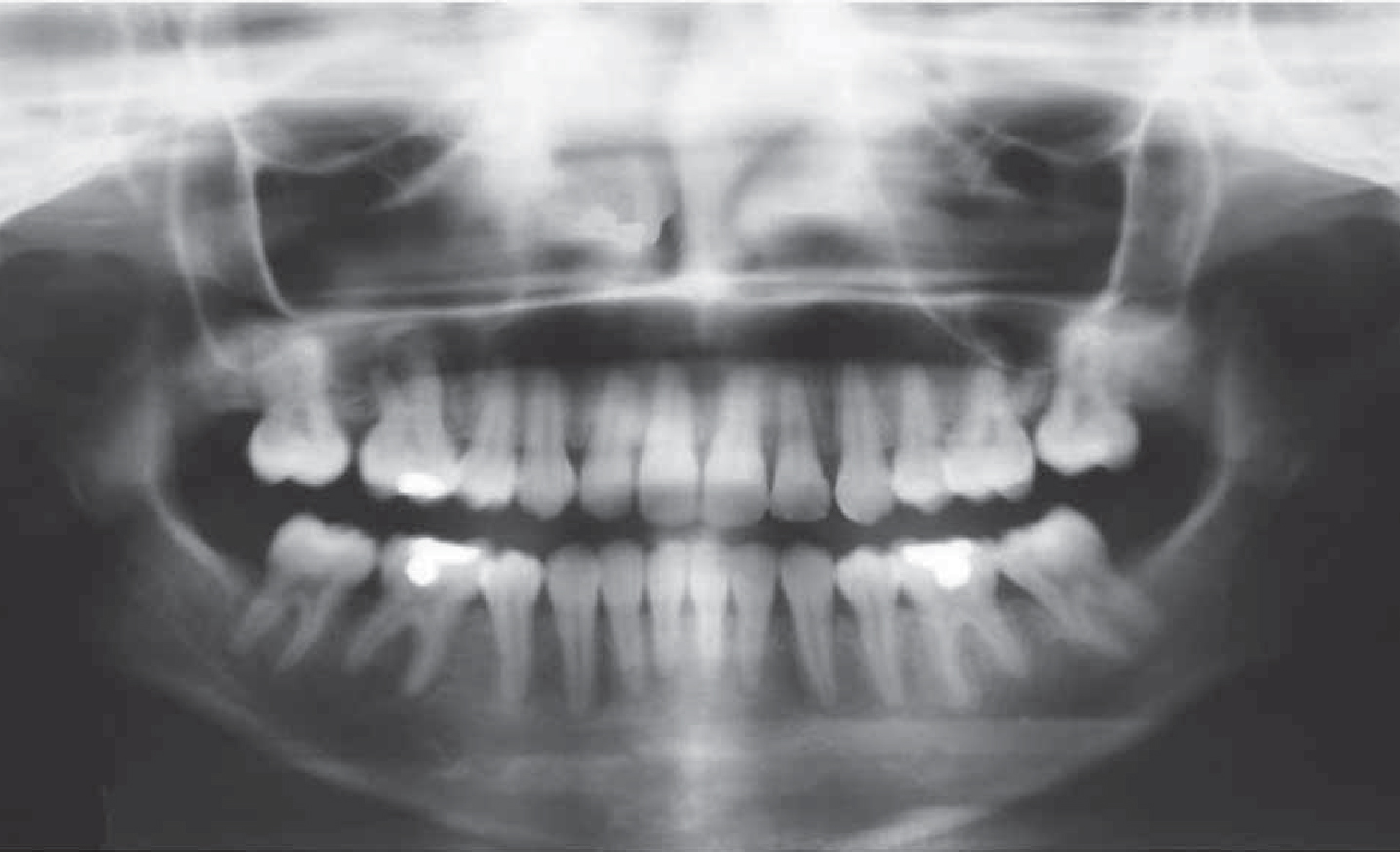
Thirteen months after the initial bracket placement, the promulgated objectives seemed to be achieved. A good Class I molar relationship was maintained along with a Class I canine relationship with the correct overjet and overbite (Figure 6). Extra-oral photographs showed a pleasing profile (Figure 7). Cephalometric analysis and superimposition (Figure 8) revealed that the hyperdivergency of the jaw bases improved from SN-GoGn 40° to 36°; FH-GoMe, 38° to 32°, MM angle from 36° to 28°, Jarabak ratio from 58.65% to 62% (Figure 9). A post-treatment panoramic radiograph confirmed complete space closure in the premolar and canine areas (Figure 10).
Figure 6. Post-treatment intra-oral photographs. Note the upper right lateral incisor was built up with composite to match the space discrepancy.Figure 7.
(a–d) Post-treatment extra-oral photographs.Figure 8. Post-treatment lateral cephalogram.Figure 9. Superimposition of cephalometric radiographs.Figure 10. Post-treatment panoramic film.
The retention regime of the patient was implemented by instructing the patient to wear a maxillary and mandibular full wraparound Begg retainer for 24 hours a day for 2 years, followed by night-time only for another 6 months (Figure 11).
The utilization of implant anchorage has proved to have many striking features and advantages:15
The ability to provide treatment possibilities and alternatives that were not previously viable;
‘Absolute’ anchorage leads to a more reliable treatment plan and enables a reduction in the treatment time as a consequence of avoiding round tripping;
This anchorage system obviates the need for patient compliance. Extra-oral anchoring devices, such as headgear, could be replaced by this method unless the utopia of absolute patient co-operation could be consistently obtained.
In the present case, high pull headgear with TPA was one of the alternate treatment options; the motive for using high pull headgear was to conserve anchorage and also to intrude the molars, however, the patient refused this option. The second alternative was to submit the patient to orthognathic surgery with the associated morbidity. The patient refused the second alternative treatment option as well. Therefore, TADs offered the best non-compliant, minimally invasive, cost-benefit effective treatment alternative and offered an effective therapy for the severe bimaxillary protrusion and hyperdivergence.
The patient's complaints, which included forwardly placed upper and lower front teeth and difficulty of lip closure, were addressed very well by this treatment modality. Since the bimaxillary proclination was corrected by complete retraction of the upper and lower anterior teeth, the upper lip assumed a more relaxed inferior position. Along with the abovementioned correction, TADs also brought about good vertical molar control.
Conclusion
In conclusion, an adult critical anchorage case of severe bimaxillary protrusion was successfully treated utilizing TADs for anchorage. TADs were used as an alternative treatment to headgear or orthognathic surgery, resulting in good occlusion with a Class I molar and canine relationship. The present case indicated that the skeletal anchorage is of great importance in achieving formulated objectives in the hitherto complex maximum anchorage scenario.