Proffit WR, White RP, Sarver DM.St Louis, MO: Mosby; 2003
Cunningham SJ, Hunt NP, Feinmann C. Perceptions of outcome following orthognathic surgery. Br J Oral Maxillofac Surg. 1996; 34:210-213
Nurminen L, Pietilä T, Vinkka-Puhakka H. Motivation for and satisfaction with orthodontic-surgical treatment: a retrospective study of 28 patients. Eur J Orthod. 1999; 21:79-87
Luther F, Morris DO, Hart C. Orthodontic preparation for orthognathic surgery: how long does it take and why? A retrospective study. Br J Oral Maxillofac Surg. 2003; 41:401-406
Nagasaka H, Sugawara J, Kawamura H, Nanda R. “Surgery first” skeletal class III correction using the Skeletal Anchorage System. J Clin Orthod. 2009; 43:97-105
Dowling PA, Espeland L, Krogstad O, Stenvik A, Kelly A. Duration of orthodontic treatment involving orthognathic surgery. Int J Adult Orthod Orthognath Surg. 1999; 14:146-152
Diaz PM, Garcia RG, Gias LN Time used for orthodontic surgical treatment of dentofacial deformities in white patients. J Oral Maxillofac Surg. 2010; 68:88-92
Luther F, Morris DO, Karnezi K. Orthodontic treatment following orthognathic surgery: how long does it take and why? A retrospective study. J Oral Maxillofac Surg. 2007; 65:1969-1976
Robb SI, Sadowsky C, Schneider BJ, BeGole EA. Effectiveness and duration of orthodontic treatment in adults and adolescents. Am J Orthod Dentofacial Orthop. 1998; 114:383-386
Flanary CM, Alexander JM. Patients' response to the orthognathic surgery experience: factors leading to dissatisfaction. J Oral Maxillofac Surg. 1983; 41:770-774
Wilcko WM, Wilcko T, Bouquot JE, Ferguson DJ. Rapid orthodontics with alveolar reshaping: two case reports of decrowding. Int J Periodontics Restorative Dent. 2001; 21:9-19
Villegas C, Uribe F, Sugawara J, Nanda R. Expedited correction of significant dentofacial asymmetry using a “surgery first” approach. J Clin Orthod. 2010; 44:97-103
The combined treatment of orthognathic surgery with orthodontics for severe skeletal malocclusion can dramatically improve facial aesthetics. The traditional treatment plan for a skeletal malocclusion is orthognathic surgery, including a pre-orthodontic and post-orthodontic phase. Pre-orthodontic treatment increases the total treatment time and is sometimes considered the worst part of the treatment by the patient. Surgery followed by orthodontic treatment gives a good result and reduces the treatment duration for certain selected cases. The purpose of the present study was to report our experience with the ‘Surgery First’ approach for skeletal malocclusions.
CPD/Clinical Relevance: Skeletal malocclusions where the dental discrepancy is not severe can be treated first with orthognathic surgery followed by orthodontic treatment. This may reduce the overall treatment time.
Article
Traditional orthognathic treatment has consisted of a variable length of pre-operative orthodontic preparation, the surgery itself, and a relatively constant period of post-operative orthodontics.1 Patients have usually expressed high levels of satisfaction with the aesthetic and functional outcomes, especially if they have been accurately informed about all aspects of their treatment.2 However, a significant percentage of patients will rate the orthodontics as the worst part of their treatment due to the appliances’ visibility, the pain caused, and the duration.3 The estimated duration of orthodontic treatment has often tended to be too optimistic.4
Recently, the utilization of surgery without orthodontic preparation (ie ‘Surgery First’), followed by regular post-operative orthodontic alignment, was proposed by Nagasaka et al.5 The authors used this approach to correct skeletal Class III malocclusion with the aid of skeletal anchorage system orthodontics. The total treatment time was noticeably reduced. In addition, pre-operative profile worsening owing to incisor decompensation was avoided and the immediate profile improvement after the surgery was greatly appreciated by the patient.5
Case report
Pretreatment evaluation
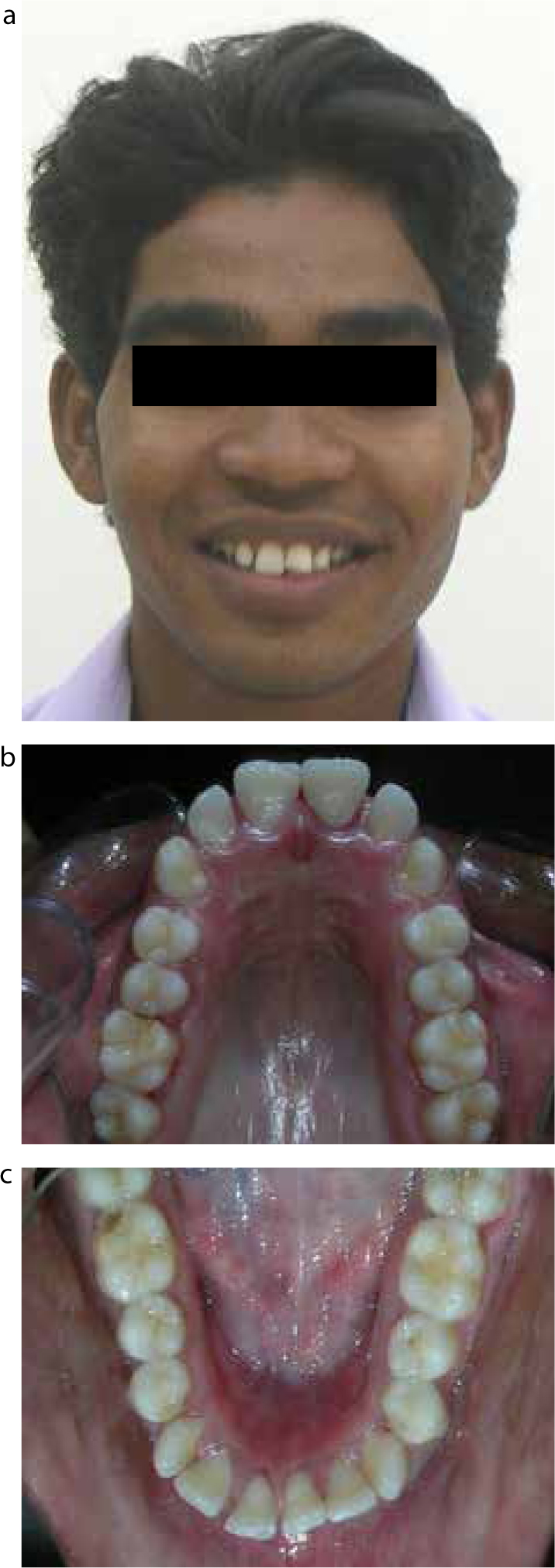
A 21-year-old male patient reported to the orthodontic clinic with the chief complaint of forward placed upper front teeth. Extra-oral examination revealed that the patient had an apparently symmetrical mesoprosopic face, potentially incompetent and protruded lips with more protrusion of the lower lip, an interlabial gap of 6 mm and an incisal display of 4.5 mm at rest. His smile was a consonant type with 100% upper incisor and 3.5 mm of upper gingiva visible (gummy smile) (Figure 1a).
Figure 1.
(a–d) Pre-surgical extra-oral and intra-oral views.
Intra-oral examination revealed a full complement of permanent teeth except the third molars on the left side. The periodontium appeared healthy. Both upper and lower incisors were proclined with mild spacing in the upper arch anterior segment (Figure 1b–d). There was mild crowding in the lower anterior segment. Overjet and overbite was increased, with a Class I molar and canine relation on both sides. The upper left central incisor was fractured and the upper midline was not coincident with the lower.
Examination of study models showed an overjet of 6 mm and an overbite of 4 mm. The Curve of Spee was 4.5 mm with a space discrepancy in the upper arch of 24 mm and in the lower arch of 20 mm. Radiographic examinations showed Class II skeletal bases with both jaws prognathic. Both maxillary and mandibular incisors were proclined. The soft tissue analysis revealed significantly protrusive upper and lower lips in relation to the E line with a severely decreased nasolabial angle.
Treatment plan
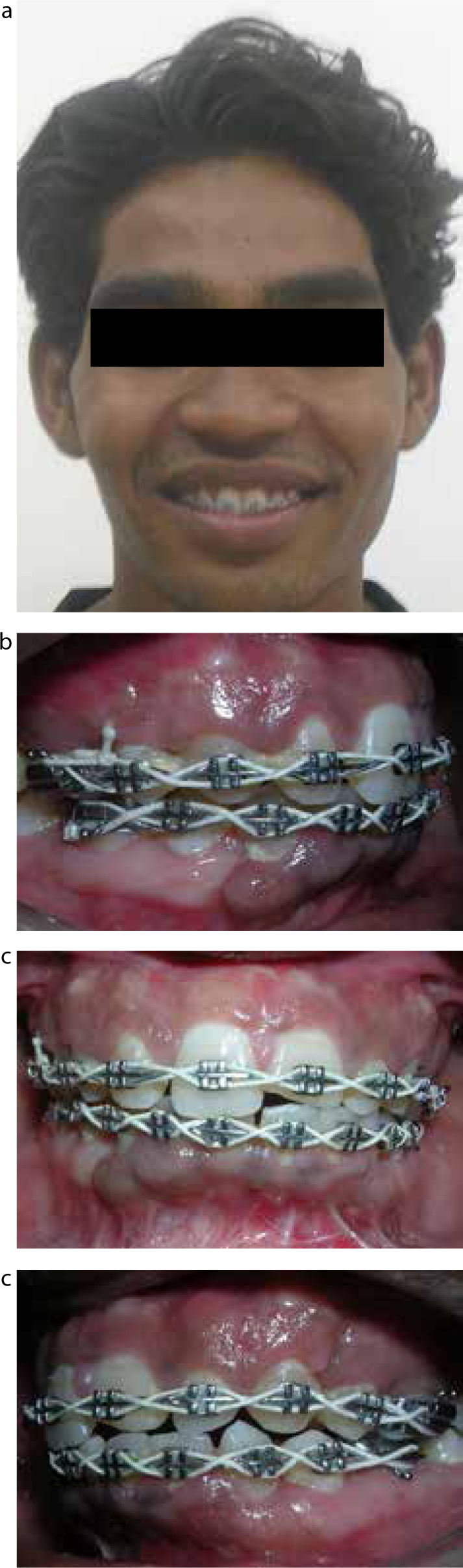
The virtual orthodontic set-up ruled out the need for extractions and verified the adequate position and axial inclination of the upper incisors. The virtual surgical treatment plan included a Le Fort I maxillary osteotomy with a 8 mm setback, with superior repositioning and subapical anterior osteotomy in the lower jaw with 7mm of setback and the extraction of bilateral upper and lower first premolars. His post-operative recovery was uneventful, and the patient was discharged from the hospital after 4 days (Figure 2a–c). His orthodontics began a month later with a Standard Edgewise technique – 0.018”slot – after surgery and involved arch alignment and levelling, with decompensation of the lower arch (Figure 3a–d).
Figure 2.
(a–c) Post-surgical extra-oral and intra-oral views.Figure 3.
(a–d) Post-orthodontic extra-oral and intra-oral views.
Result
The total orthodontic treatment required was 6 months to achieve an improved profile, relieving crowding and space closure. Proclination of jaws and anterior teeth was reduced with the result of normal overjet and overbite. Class I molar and canine relationship was retained. Radiographic changes seen after surgery included a decrease in SNA, SNB, upper incisor to NA, lower incisor to NB and the nasolabial angle. Intercanine and intermolar width was maintained after the completion of orthodontic treatment (Figures 3a–d).
Patient expressed satisfaction with the duration and results of treatment as 100 on the visual analog scale. We considered the case easy and extremely satisfactory from a time-results and patient-perception perspective.
Discussion
The ‘Surgery First’ concept in orthognathic surgery was introduced by Nagasaka et al in 2009. They reported the correction of a Class III skeletal malocclusion with mandibular setback surgery and subsequent orthodontic alignment with the aid of temporary anchorage devices. The patient did not undergo any previous orthodontic preparation.5 Because of their excellent clinical results and substantial reduction in total treatment time, the investigators postulated that this new treatment approach could become a standard procedure in the future. Taking into consideration the number of patients requesting orthognathic surgery for primarily aesthetic concerns and time limitations for long treatment, the ‘Surgery First’ approach could represent a reasonable, cost-effective method to manage skeletal maloclusion in selected cases.
Traditional surgical-orthodontic treatment has included two orthodontic phases: a pre-operative preparation in which most of the orthodontic movements are performed to achieve a precise, stable occlusion and a post-operative phase for minor adjustments. Pre-operative orthodontic treatment usually lasts 15 to 17 months,4,6 or even up to 24 months.7 However, the total pre-operative treatment is frequently longer than that initially indicated to the patient.4 The average duration of the post-operative orthodontic phase has varied from 7 months8 to 12 months.9 No statistically significant differences regarding patient age, gender, or type of malocclusion have been detected.4,7,8,9 These orthodontic phases often cause significant discomfort to the patient.4,10 One study found that one-third of patients rated the orthodontics as the worst part of their orthognathic treatment owing to the visibility and discomfort of the appliance and the length of treatment.3 In contrast, if the surgery is performed before the orthodontic treatment, the total treatment time will be noticeably reduced. Nagasaka et al5 reported that the treatment could be shortened to about 12 months, less than the average time needed for traditional pre-operative orthodontics alone.4,7,8 In the present case, the total treatment time was 180 days. These data, although lacking statistical significance, have illustrated that a ‘Surgery First’ approach tends to condense the treatment time considerably, mainly by shortening the total orthodontic period.
In 2001, Wilcko et al suggested that rapid tooth movement in the context of corticotomy-facilitated orthodontics was the result of a demineralization–remineralization process consistent with the wound healing pattern of the regional acceleratory phenomenon.11 It seems that selective bone injury results in an overwhelming activating stimulus for both catabolic and anabolic responses in the periodontium.12 It is possible that the alveolar bone adjacent to the osteotomies performed during orthognathic surgery also undergoes increased bone turnover. This could account for the more efficient post-operative orthodontic movements and hence contribute to the total treatment time reduction in a ‘Surgery First’ sequence.12 Moreover, routine pre-operative orthodontics involves dental alignment, arch co-ordination, and incisor decompensation; very often, the latter tends to prolong the treatment time with little or no significant benefit to the patient.5 In addition, axial correction of the incisors exacerbates an anterior crossbite and tends to unmask the patient's underlying skeletal deformity. Especially in the case of Class III patients, the prognathic profile will be greatly accentuated as the pre-operative orthodontics progresses. This intensifies the patient's perception of facial disharmony. The ‘Surgery First’ approach, in contrast, corrects the skeletal problem (and hence the aesthetic concern) from the outset. This clearly accounted for the favourable evaluation of the treatment by our second patient.
Another advantage of the ‘Surgery First’ approach compared with traditional surgical-orthodontic treatment includes the rapid profile improvement with subsequent immediate patient satisfaction. In contrast, several difficulties and disadvantages must be considered. First, the occlusion cannot serve as a guide for the designation of treatment goals. Secondly, the immediate post-operative occlusion is often unstable; thus, an occlusal splint while eating has been recommended.5 Temporary anchorage devices can be considered to help stabilize the osteotomies when no solid orthodontic appliances are present during surgery.5,11
This treatment concept requires a precise diagnosis and detailed treatment planning. The post-operative orthodontic movements must be accurately planned with the surgical plan, implying constant communication between the surgeon and orthodontist. It is important that the orthodontist be skilled in orthognathic surgery cases, because the orthodontist is often confronted with a rather complex scenario.
Conclusion
A thorough diagnosis, planning, and execution could render the ‘Surgery First’ approach appropriate for a significantproportion of our routine cases.