Suri L, Gagari E Delayed tooth eruption: pathogenesis, diagnosis, and treatment. A literature review. Am J Orthod Dentofacial Orthop. 2004; 124:432-445
Nolla CM The development of the human dentition. ASDC J Dent Child. 1960; 27:254-266
O'Connell AC, Puck JM, Grimbacher B Delayed eruption of permanent teeth in hyperimmunoglobulinemia E recurrent infection syndrome. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000; 89:177-185
Moretti de Lima A, Arantes Sperandio V, Pereira da Rocha S Do you know this syndrome?. An Bras Dermatol. 2013; 88:836-838
Grimbacher B, Holland SM, Puck JM Hyper-IgE syndromes. Immunol Rev. 2005; 203:244-250
Kamasaki Y, Hidaka K, Nishiguchi M, Fujiwara T Dental manifestations of a pediatric patient with hyperimmunoglobulin E syndrome: a case report. J Dent Child. 2012; 79:100-104
Holland SM, DeLeo FR, Elloumi HZ STAT3 Mutations in the hyper-IgE syndrome. N Engl J Med. 2007; 357:1608-1619
Laurent J, Noirot C, Ansquer JC How to define the normal level of serum IgE in adults?. Ann Med Interne (Paris). 1985; 136:419-422
Grimbacher B, Holland SM, Gallin JI Hyper-IgE syndrome with recurrent infections – an autosomal dominant multisystem disorder. N Engl J Med. 1999; 340:692-702
Freeman AF, Holland SM Clinical manifestations, etiology, and pathogenesis of the hyper-IgE syndromes. Pediatr Res. 2008; 65:32R-37R
Cohen-Solal M, Prieur AM, Prin L Cytokine-mediated bone resorption in patients with the hyperimmunoglobulin E syndrome. Clin Immunol Immunopathol. 1995; 76:75-81
Welbury R, 4th edn. New York: Oxford University Press; 2001
Frank CA Treatment options for impacted teeth. J Am Dent Assoc. 2000; 135:623-632
Becker A, Lustmann J, Shteyer A Cleidocranial dysplasia: Part 1 – General principles of the orthodontic and surgical treatment modality. Am J Orthod Dentofacial Orthop. 1997; 111:28-33
Doruk C, Bicakci AA, Babacan H Orthodontic and orthopedic treatment of a patient with incontinentia pigmenti. Angle Orthod. 2003; 73:763-788
Tsuchiya Y, Sueishi K, Yatabe K, Yamaguchi H A case of Antley-Bixler syndrome with severe skeletal Cl. III malocclusion. Bull Tokyo Dent Coll. 2003; 45:87-93
Orthodontic management of delayed permanent tooth eruption and a case report of hyper-IgE syndrome Nabeel Bhatti Pratik K Sharma Orthodontic Update 2025 10:1, 24-27.
Authors
NabeelBhatti
BDS MBBS, MFDS MRCS
StR Oral and Maxillofacial Surgery, Oral and Maxillofacial Department, The Royal London Hospital E1 1BB
Senior Clinical Lecturer and Consultant Orthodontist, Department of Orthodontics, Centre for Oral Growth and Development, Barts and The London School of Medicine and Dentistry, Queen Mary University of London, E1 4NS, UK
This article aims to look at the treatment and management of patients presenting with delayed tooth eruption of the permanent dentition. We describe the case of a 17-year-old girl who presented having been diagnosed with Hyper-IgE syndrome. The patient was positive for the STAT-3 gene and presented with a history of some classic Hyper-IgE features. There was a history of multiple skin abscesses and she was on long-term antibiotics. She presented in the mixed dentition with multiple retained deciduous teeth and a full complement of unerupted and fully formed permanent teeth. This article will describe features of this syndrome and discuss management strategies for patients presenting with delayed eruption.
Clinical Relevance: This case study highlights the difficulties in managing patients who present with retained primary dentition at an older age. It also presents a rare case presentation of a patient with Hyper-IgE.
Article
Delayed tooth eruption (DTE) is a term described as the ‘emergence of a tooth into the oral cavity at a time that deviates significantly from norms established for different races, ethnicities, and sexes’.1 In general, the causes for delayed eruption are unknown but the literature does detail specific conditions (Table 1) that are often associated with it.2 The eruption of teeth is a sequential process and deviations from the normal sequence can be separated into genetic and environmental causes.3
Cleidocranial dysplasia
Turner's syndrome
Gardner's syndrome
Down's syndrome
Apert's syndrome
Ectodermal dysplasia
Vitamin D-resistant rickets
de Lange's syndrome
Mucopolysaccharidosis
Endocrine disorders
Hypothyroidism
Hypopituitarism
Hypoparathyroidism
Epidermolysis bullosa
Prematurity/low birth weight
Ichthyosis
Cherubism
Pyknodysostosis
Drug-induced gingival overgrowth
Hereditary gingival fibromatosis
Gross nutritional deficiency
Hyperimmunoglobulin E syndrome
There are two distinct processes which are involved in the eruption of permanent teeth. One is the intra-bony tooth formation process and the other is the eruption process itself. One study shows that the delay in establishment of the permanent dentition is not due to delay in primary teeth eruption nor delay in permanent tooth development. Instead, it suggests that the presence of the primary dentition due to failure of exfoliation may be the contributing factor.4
Hyper-Immunoglobulin E syndrome (also known as Job's or Buckley's syndrome) is a rare inherited primary immunodeficiency condition, in which serum levels of Immunoglobulin-E (IgE) are extremely elevated.4,5 Available literature suggests that 72% of Hyper-IgE patients exhibit unexplained retention of the primary dentition with lack of root resorption.6
Hyper-IgE is clinically characterized by recurrent staphylococcal and Haemophilus influenzae infections of the skin, often presenting as abscesses.7 This presentation can often be the triggering factor to this diagnosis. It is also common for patients to have mucocutaneous candidiasis along with recurrent staphylococcal, Aspergillus and pneumocystis lung infections.5 Patients may also present with multiple warts of viral origin, often around areas of dermatitis and eczema.
These patients are at high risk of infections due to a mutation on the Signal Transducer and Activator of Transcription three gene (STAT-3), which is involved in the transduction of signals for the production of cytokines involved in control of fungal and bacterial infections.8 Hyper-IgE is characterized immunologically with peripheral eosinophilia and elevated serum levels of IgE up to 10 times the normal levels. The normal upper limit of IgE is between 150 and 300 UI/ml.9 In Hyper-IgE, levels of >2000 UI/ml are seen.10
Clinical management of patients often involves long-term antibiotic and antifungal therapy, along with aggressive treatment of any active infections.4 Abnormal skeletal characteristics include hyper-extensibility of joints along with spinal deformities such as scoliosis.11 Facial and cranial abnormalities include prominent supra-orbital and frontal ridges, along with broad noses. Hyper-IgE is thought to cause cytokine-mediated bone resorption, which can lead to pathological fractures.12
Other oral features related to Hyper-IgE are high vaulted palates in 36% of patients, oral candidiasis in 82% of patients and 38% under 17 years of age have angular cheilitis.4
History
A 17-year-old female presented as a tertiary referral to the orthodontic clinic at The Royal London Hospital. She had been diagnosed with Hyper-IgE from a young age after presenting with painless large abscesses requiring incision and drainage, along with admission for intravenous antibiotics. She had been tested positive for the STAT-3 gene, however presented with mild symptoms. Relevant medical history included birth at 36 weeks with a low birth weight. Her mother contracted chicken-pox during pregnancy and, on presentation, she was on long-term prophylactic Flucloxicillin. There was no reported history of this condition amongst her parents or siblings.
The reason for referral was for a joint orthodontic/surgical opinion to identify if her case would benefit from surgical exposure and active orthodontics.
Extra-oral assessment
The patient presented with a a skeletal I pattern with average vertical proportions. She had no asymmetries but there were multiple scars on her face and neck resulting from previous surgical drainage of skin abscesses.
During her neonatal period she showed no signs of eczema or skin rashes. However, over the following years she developed skin abscesses on her face and neck region which required drainage. Microbiological analysis of swabs taken from the abscess during subsequent drainage isolated Staphylococcus aureus. As a teenager, she presented with only one area of eczema on her leg and there was a history of a pathological fracture of her radius in childhood. Contrary to the common features, she did not have any history of recurrent thrush infections. Her highest IgE levels have been recorded at 970 IU p/L.
Intra-oral assessment
The patient presented with a Class I incisal relationship on a skeletal I pattern. She was in the mixed dentition with retained primary teeth in the buccal segments. The maxillary permanent incisors and the first permanent molar had erupted in both arches. The arches were well aligned and the dentition was in good health with no caries detected. There was one restoration in the deciduous maxillary left first molar. There were no clinical signs of ankylosis.
We noted a high vaulted palate, consistent with Hyper-IgE features. The young girl did not exhibit any of the other facial and skeletal abnormalities that can often be associated with Hyper-IgE.
Radiographic report
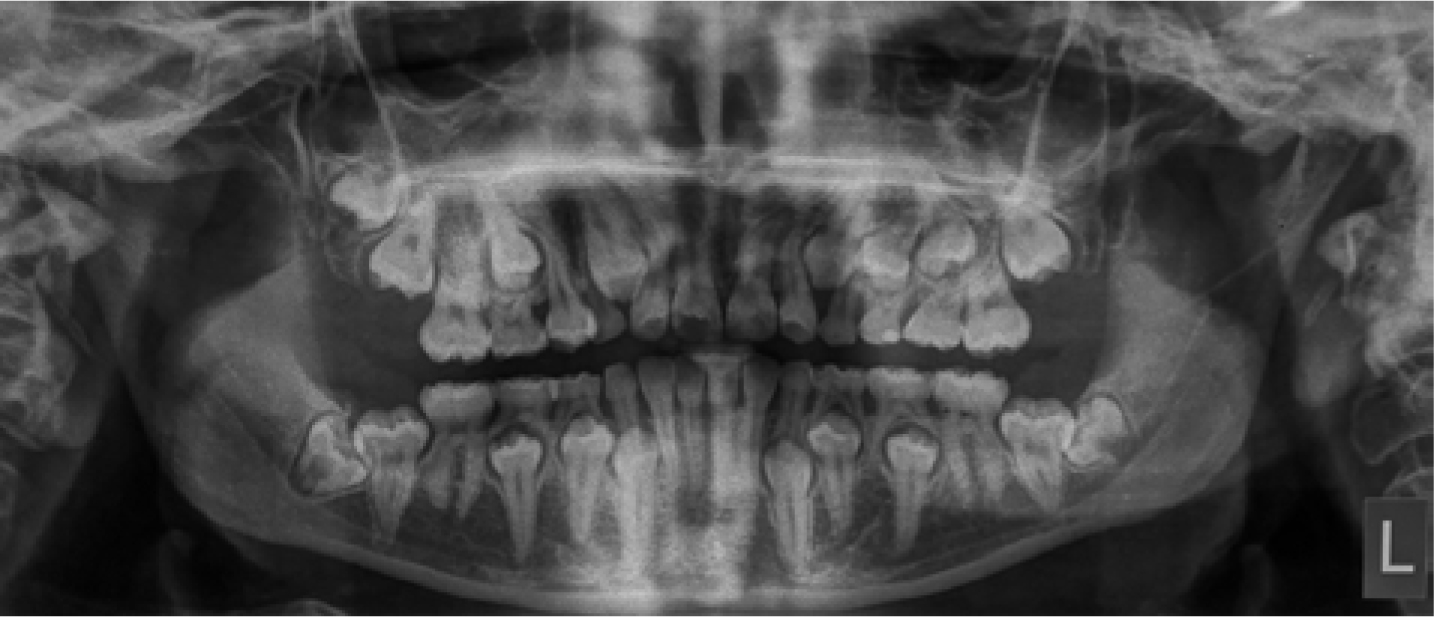
An orthopanthogram (Figure 1) and upper standard occlusal radiograph (Figure 2) were undertaken to demonstrate her dental development.
Figure 1. OPG showing the presence of a mixed dentition with root erupted incisors and first permanent molars alongside root resorption on deciduous teeth.Figure 2. Upper standard occlusal: no obstructive supernumeries are present.
The OPG indicated no bony abnormalities in either the mandible or maxilla. It revealed a full complement of the adult dentition with the exception of a congenitally absent maxillary left third molar. The lower third molars exhibited mesio-angular impactions. The roots of the primary dentition showed positive signs of resorption and none of the adult dentition showed radiographic signs of ankylosis. The permanent dentition showed successful root formation.
Along with the OPG, the upper standard occlusal confirmed no ectopic tooth nor any supernumerary in the anterior maxilla.
Treatment
The treatment decision in view of the presentation was conservative management. It was decided to monitor and review her developing dentition in one year's time as the primary dentition showed evidence of root resorption radiographically. If, in the future, there was little progression towards establishment of the permanent dentition, then sequential quadrant extractions of primary teeth could be considered, along with orthodontic treatment to align the permanent dentition. The main reason for a conservative approach being taken was due to the good health, alignment and function of her primary dentition.
Discussion
Delayed eruption can be caused by systemic or local causes. Local mechanical causes are the most common cause, such as ankylosis, supernumerary teeth, crowding and soft tissue impactions, alongside cyst and tumour formations.13 In general, chromosomal abnormalities are known to be associated with it, however, other environmental factors, such as gross nutritional deficiencies, can also be implicated.14
Treating patients with delayed eruption of the secondary dentition has been documented, often with reference to more common hereditary conditions, such as cleido-cranial dysplasia, or with local causes, such as ectopic canines.
There are different methods that are used in the treatment of such cases. They are all based upon the eruption sequence. The ideal method in such a case presenting with little functional and aesthetic concern was to intervene as little as possible. Treatment options for the management of impacted teeth can be separated into four categories:
The following methods have been described over the years for management of failed eruption of permanent teeth and encompass the four categories above in their various forms.
Permanent incisors are exposed and the area is packed. Once healed the permanent incisors are bonded with extrusive attachments
3
9–10
Deciduous posterior teeth are removed
4
9–12
Premolars are surgically exposed and supernumerary teeth are removed and the area is packed. Once healed the premolars and canines are bonded with extrusive attachments
This method involves serial surgical procedures at various ages determined by permanent tooth formation16 and entails multiple surgical episodes over many years that may present with compliance issues. It also requires the placement of healing packs that can interfere with normal function, such as eating, and possibly increase local risk factors for infection.
The aim of this approach is to remove all deciduous and supernumerary teeth along with exposure and bonding of attachments in a single surgical episode. Packs are placed and only the soft tissue is closed. They are changed regularly until orthodontic brackets can be placed on the erupting teeth.
Owing to the healing period required, there is considerable delay in the orthodontic extrusion of the permanent teeth. The single procedure does mean that the posterior molars may have immature root formation prior to exposure.
This approach looks at four principles which culminate to help with the patient's self-image (Table 3) and allows for the anterior teeth and aesthetics to be established earlier with the remainder teeth being exposed and extracted at appropriate times closest to their physiological exfoliation time. It also considers the orthodontic treatment plan which can be important in cases where there are missing teeth and crowding due to early extractions.
Principle
Stage
Treatment
1
Presenting clinical features
Retained deciduous teeth, supernumerary teeth, retarded eruption, reduced lower facial height, late eruptions of 6s and serious delay of root development
2
The surgical methods required to overcome them. Two surgical procedures are often planned
Intervention 1 (7–8 years old)
Extract anterior deciduous teeth, supernumerary teeth, expose permanent incisors and bond attachments
Intervention 2 (10–11 years old)
Extraction of all remaining deciduous teeth, expose premolars and molars and bond attachments to them
3
Orthodontic treatment strategy
Arch expansion maybe be required. Is anchorage available from erupted teeth? Consider spacing if missing permanent teeth. Rigid appliance will be required to prevent distortion
4
Bring anterior teeth into arch for aesthetics
To bring into the arch the anterior teeth for aesthetic purposes by extraction of the primary and any supernumerary teeth as soon as the root development is seen radiographically
Orthodontic treatment can be required when a patient presents with functional or aesthetic concerns and these should be addressed as soon as appropriate. Case reports have been described in other conditions where patients present with delayed eruption, such as Incontinentia pigmenti, an uncommon hereditary condition presenting with dental manifestations in 90% of cases. The main dental presentations include delayed eruption, partial anodontia, microdontia and peg-shaped teeth. Treatment, in such cases, includes standard orthodontic approaches such as space creation, alignment and correction of midline shifts with fixed appliance therapy.17
The skeletal pattern should also always be considered in patients presenting with hereditary conditions. The patient described in this article presented with a skeletal I base and a Class I incisor relationship. However, in some conditions there are situations where skeletal growth is also affected and, depending on the severity and unpredictability, the proposed methods described above may need to be modified. It may require multiple interventions over a period of time. A case described with Antley-Bixler syndrome presented with craniosynostosis and mid-face hypoplasia on a skeletal III base. In this case, the orthodontic treatment was limited by the cranial formation after the various operations that were proposed. In this particular case, the orthodontic treatment would evolve as the patient grew to take into consideration the skeletal pattern of growth. Therefore, applying one of the previously described approaches would not work effectively as that patient's dental and skeletal growth may not be in synchronous harmony.18
Factors such as dental health are important to consider in any orthodontic case. It has been reported and well documented that patients with chronic illnesses or those who frequently require medical attention have a poorer level of oral hygiene. In some cases, this may be as a direct result of the disease (leading to the inability to brush) or contributed to by sugarsweetened medications. It is also reported that Hyper-IgE patients present with a higher number of decayed, missing or filled teeth.19 This can often lead to problems with the early loss of deciduous teeth, resulting in loss of space and the ensuing crowding. Oral hygiene is important in patients with Hype-IgE as they are at greater risk of severe infection from carious teeth due to the relative immunosuppression.7
A case describing a rare form of ectodermal dysplasia, Rapp-Hodgkin syndrome, shows that dental rehabilitation is quite involved. The 7-year-old patient in this instance presented with dental pain alongside cleft-palate, hypodontia, caries and delayed eruption. Such cases are important to identify teeth that are strategically required and, in view of hypodontia, the need to ensure that all appropriate teeth are saved to maintain function and aesthetics.20
The rather ironic presentation of the patient described in this article was of a very functional and aesthetically pleasing mixed dentition. This complicates the decision-making process. In view of keeping interventional treatment to a minimum, the approach adopted was to wait and see if the natural resorption process would exfoliate these teeth. One of the stages from the Jerusalem Approach had been completed naturally by the exfoliation of the anterior teeth and the permanent dentition had taken their place. The continued monitoring for this patient's case will include further assessment of her dental exfoliation and eruption alongside skeletal growth to ensure that the changes are favourable.