The incidence of permanent canines failing to erupt in the mandible is not as common, and, therefore, not as well reported, as that in the maxilla. Mandibular canines have important functional and aesthetic purposes and knowledge of this uncommon condition is essential for those involved with the management of these cases. This article explores the aetiology, assessment and treatment options available to manage this condition, using examples from treated cases within our department.
CPD/Clinical Relevance: An understanding of the aetiology, assessment and various treatment options available to manage impacted and transmigrated mandibular canines will inform better treatment planning.
Article
Impaction is defined as the failure of eruption of a permanent tooth with a completely developed root. Transmigration is thought to occur almost exclusively with mandibular canines and has been defined as migration of an impacted tooth across the midline by more than half of its length.1,2,3 Prevalence of mandibular canine impaction has been reported as ranging between 0.31% and 1.35%, while that of mandibular canine transmigration lies between 0.1% and 0.31%.4,5,6 A number of local and systematic factors have been proposed as the causes for these conditions; however, the precise aetiology is unknown (Table 1).
Trauma including mandibular fracture near site of canine eruption
Iatrogenic, including interference with prosthetic devices
Systemic factors
Hereditary conditions
Endocrine deficiencies
Cancer irradiation
Febrile illness
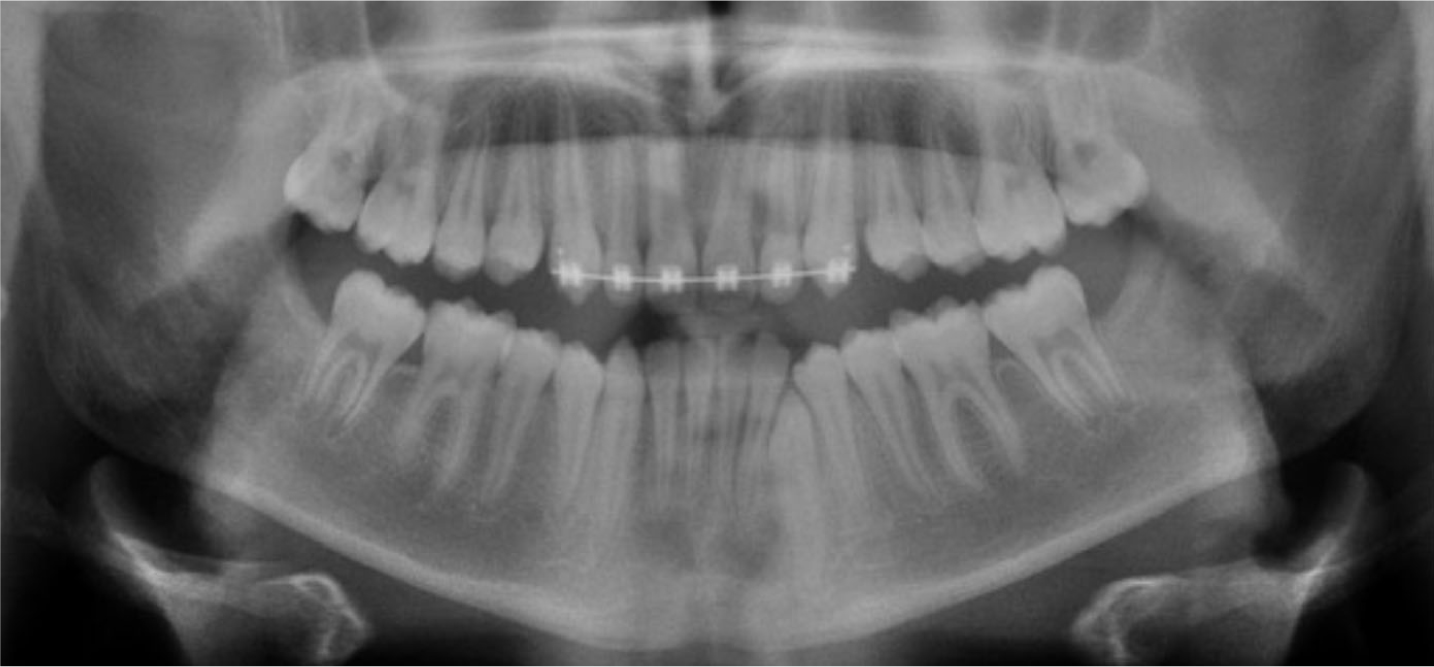
Figure 1. OPG showing an impacted LL3 due to premature loss of the LLC.Figure 2.
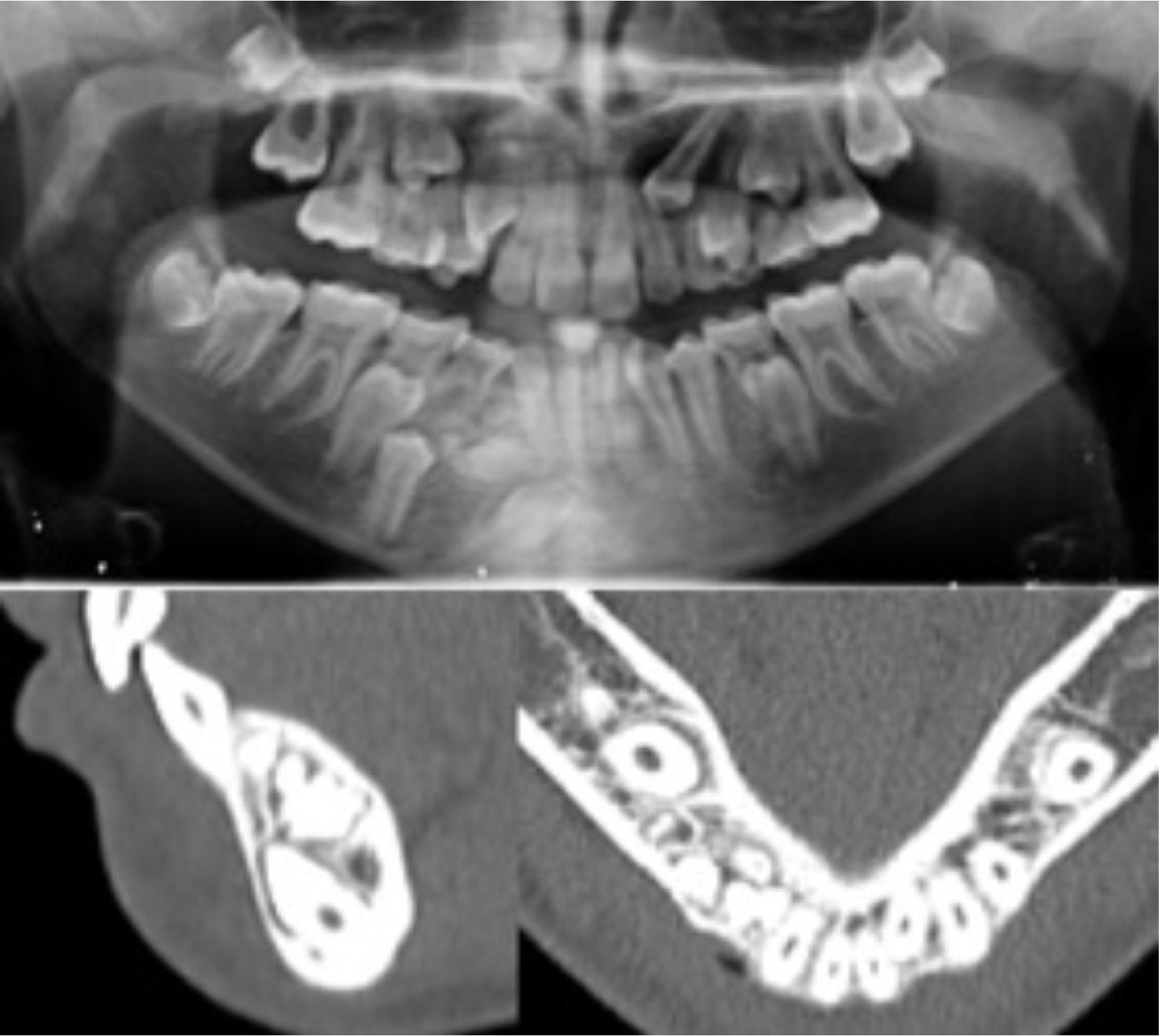
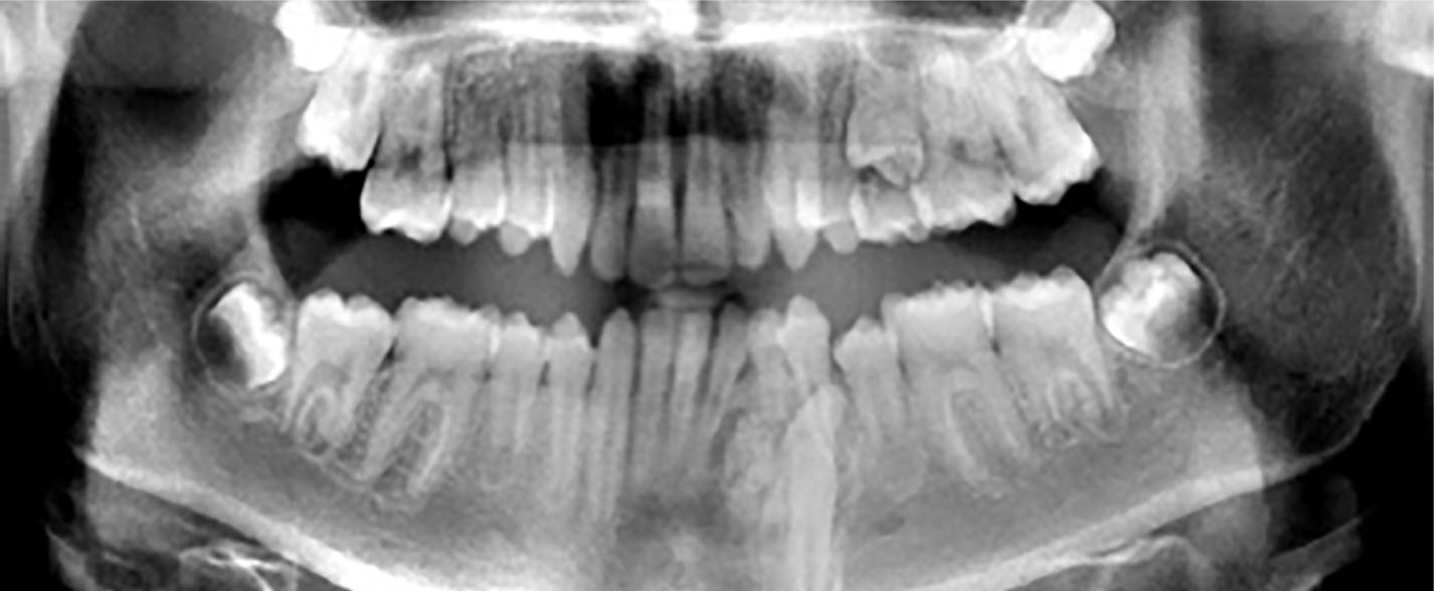
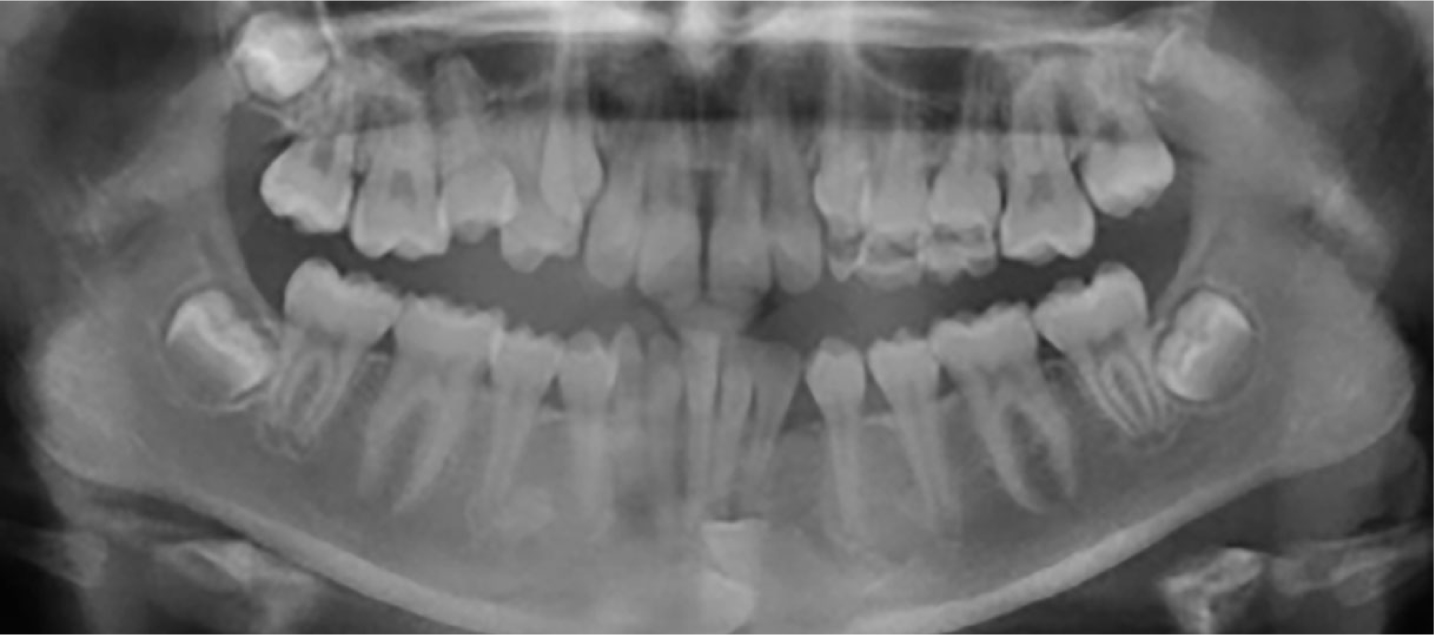
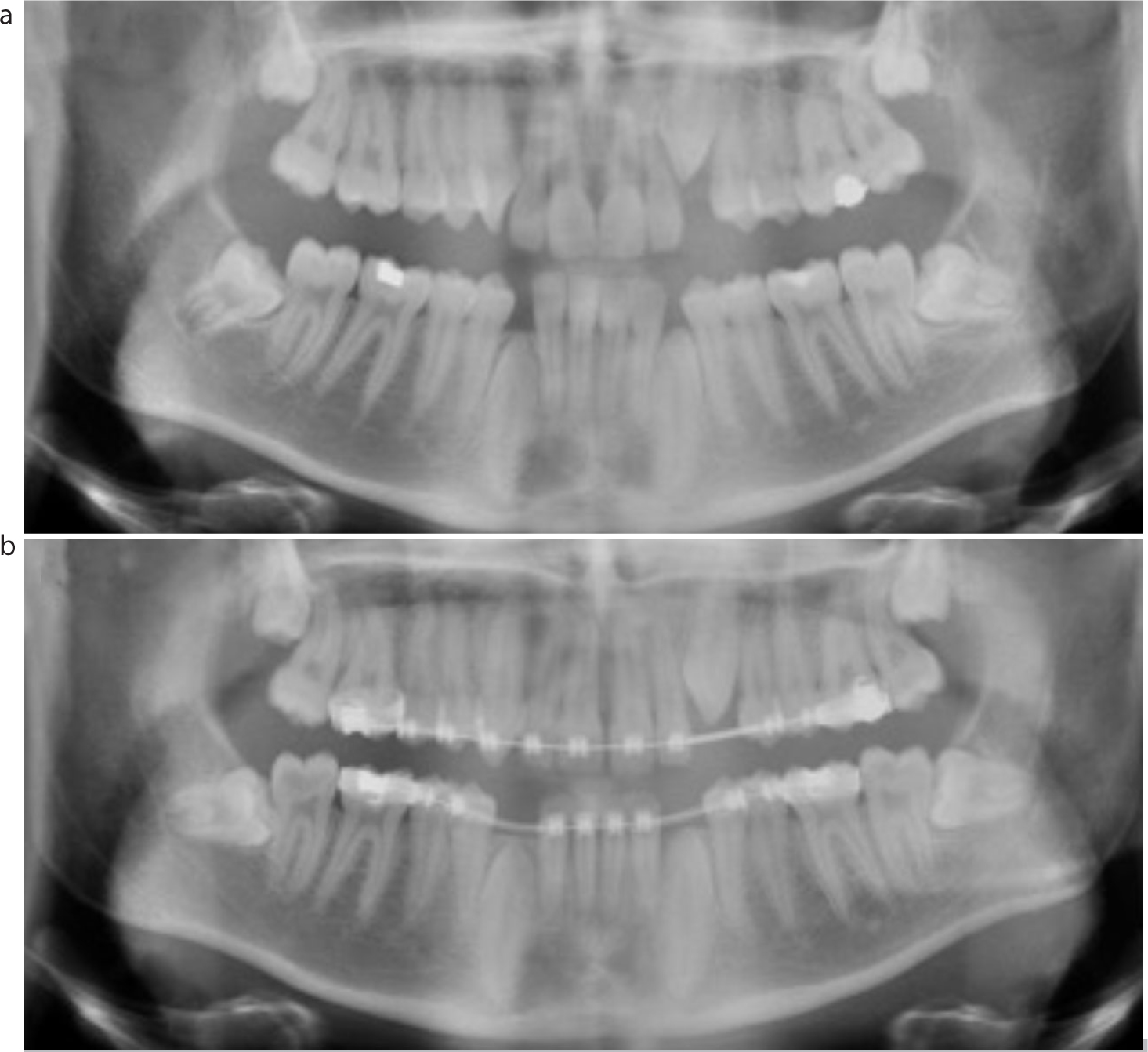
(a) OPG showing normal dental development within the mixed dentition for a 10-year-old patient, with both the LL3 and LR3 in favourable positions. (b) OPG of the same patient, at the age of 13, showing a number of retained primary teeth, in addition to significant deterioration in the position of the LL3.Figure 3. An OPG and sagittal and axial views of a CBCT scan showing impeded eruption of the LR3 caused by the presence of multiple unerupted odontomes.Figure 4. 3D view of a CBCT scan showing the presence of a complex odontome resulting in an impacted LR3.Figure 5. An OPG showing a compound odontome in the anterior mandible impeding the eruption of both the LL2 and LL3.
Although several studies have been published regarding the incidence, aetiology and treatment strategies available for unerupted maxillary canines, studies regarding mandibular canines are less common.7,8,9,10 This is partly due to the fact that failure of eruption of the mandibular canine is such a rare event, and thus clinical guidelines derived from clinical studies prove difficult to develop.
This article explores the aetiology, assessment and treatment options available to manage this condition, using examples from treated cases within our department to highlight the management of both impacted and transmigrated mandibular canines.
Assessment
Successful orthodontic treatment requires an accurate definitive diagnosis. This can be achieved with verbal history-taking, a thorough oral examination and relevant special investigations, including radiographs.
Clinical assessment
There are several clinical signs that are suggestive of mandibular canine impaction or transmigration. These signs may include:
Asymmetrical eruption of contralateral mandibular canine;
Delayed exfoliation of the primary mandibular canine;
Proclination, retroclination or displacement of the mandibular incisors;
Enlarged symphyseal area owing to the presence of the displaced mandibular canine.
To aid the clinical assessment and confirm diagnosis, special investigations may be required. These can include pulp sensibility testing using thermal and/or electric stimuli to determine whether the vitality of any adjacent teeth has been affected by the unerupted mandibular canine, percussion tests to assess the surrounding peri-apical tissues, in addition to appropriate radiographs.
Radiographic investigation
Radiographs are necessary to determine the presence and position of the unerupted mandibular canine, the condition of adjacent teeth (particularly to assess for resorption associated with the primary mandibular canine and any adjacent permanent incisors) and for any other pathology. Panoramic, lateral cephalometric, occlusal, peri-apical or submentovertex views can be used to confirm the location of the tooth. Radiographs are often taken in combination to determine the position of the unerupted canine relative to the mandibular arch, using the principle of either horizontal or vertical parallax. When the tooth position is uncertain, or a more detailed examination is required, cone-beam computed tomography (CBCT) can be indicated to provide a three-dimensional image. The need for CBCT must be balanced against increased radiation dosage; however, field limitation can help to significantly reduce the effective radiation dose.11
Treatment options
Radiographic monitoring
Symptomless, unerupted mandibular canines may remain in situ. This is often appropriate for grossly displaced transmigrated teeth, or those that are intimately related to adjacent teeth and may cause significant surgical morbidity following attempts at their removal (Figures 6 and 7). However, it is important to remember, that teeth left in situ should be periodically monitored radiographically to assess for any potential adverse changes (Table 2).
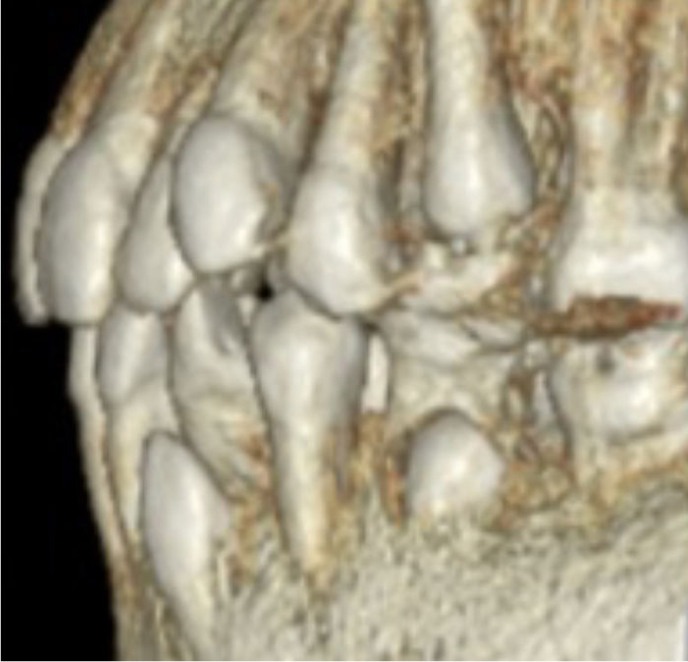
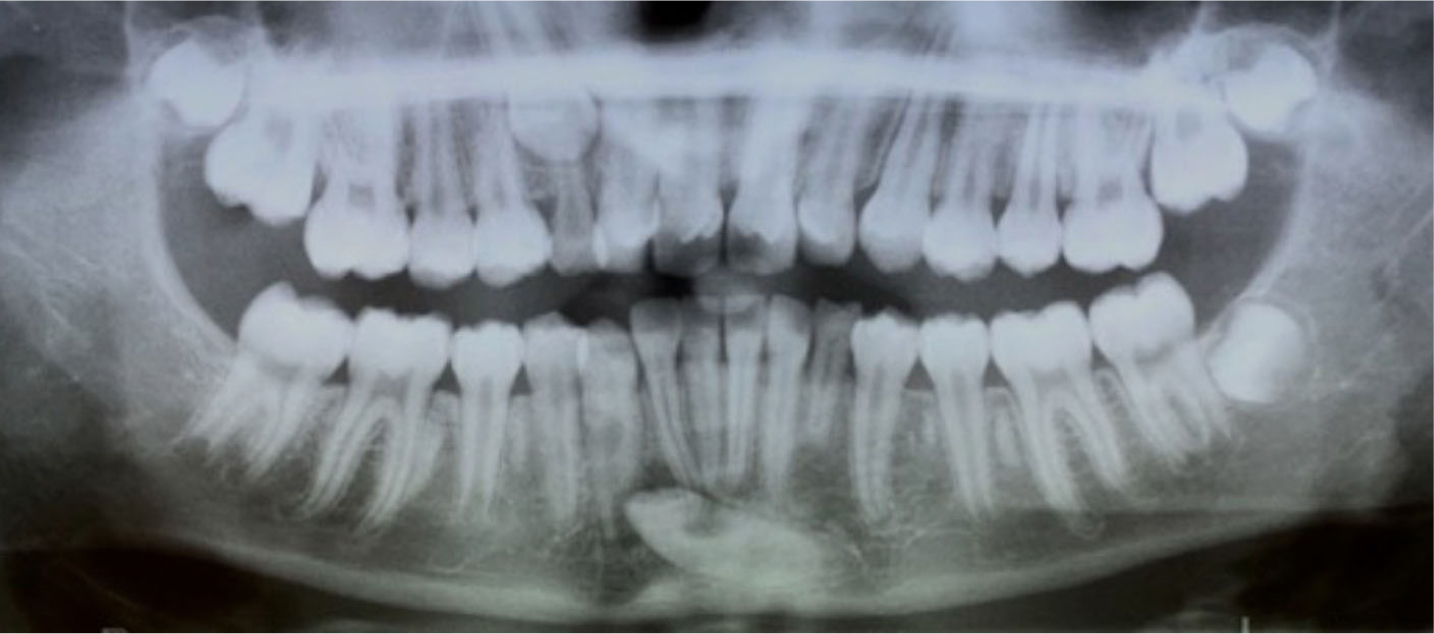
Figure 6. OPG showing transmigrated mandibular canines meeting at the midline of the mandible. Cases such as these have previously been referred to as ‘kissing canines’ or ‘mirror image canines.’12Figure 7. A 3D CBCT view showing the intimate relationship of a buccally impacted LL3 with the LL2.
Root resorption of adjacent teeth
Pathology, follicular enlargement and cystic formation (Figures 8 and 9)
Displacement or rotation of adjacent teeth (Figure 10)
Deterioration in position of unerupted tooth (Figure 11)
Periodontal damage
Prosthetic issues
Neuralgic symptoms
Prevention of orthodontic movement
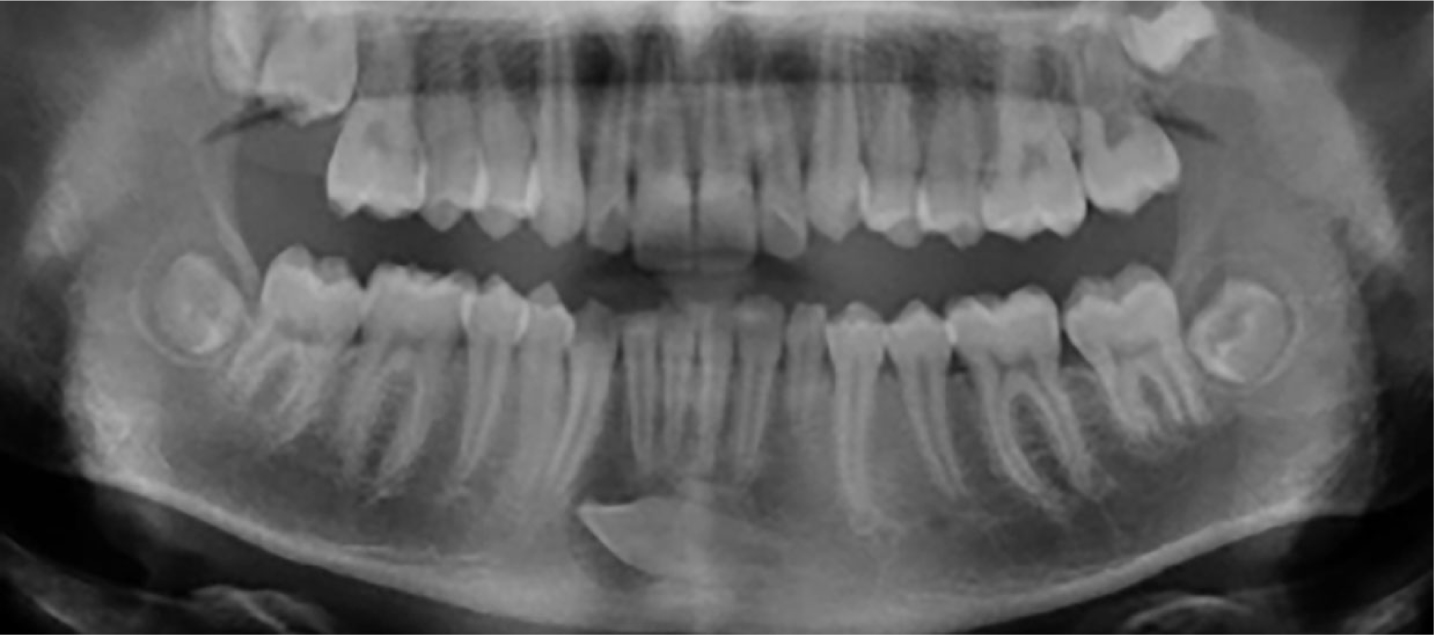
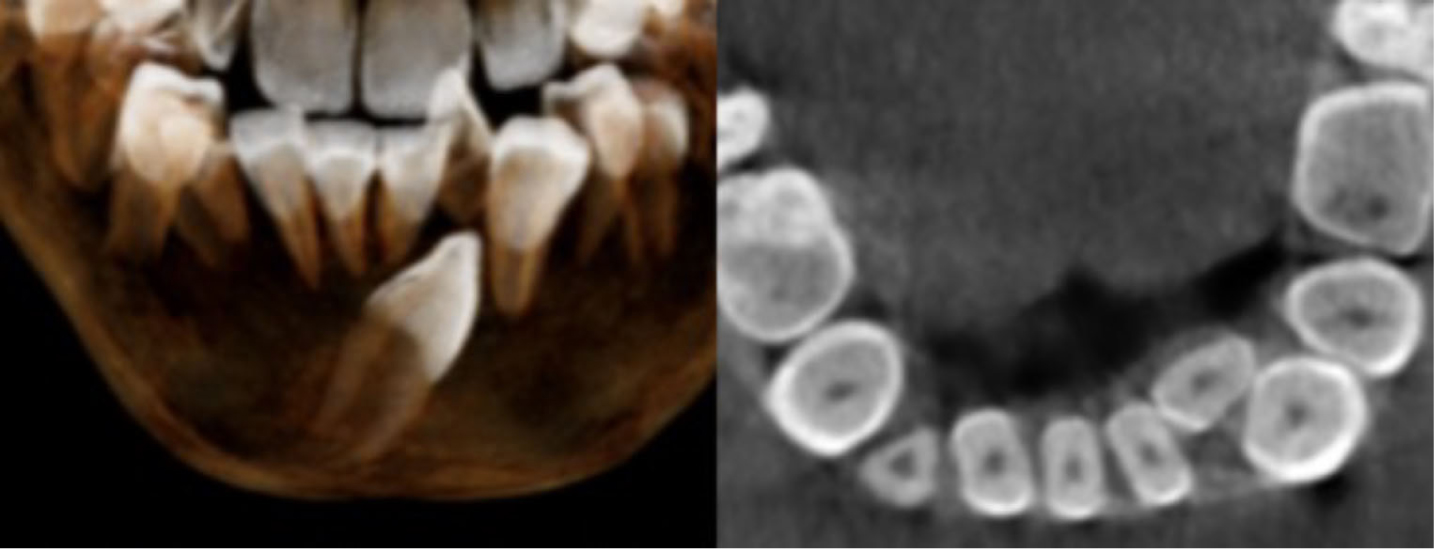
Figure 8. An OPG showing a transmigrated LL3 with evidence of cystic change.Figure 9. An OPG of a similar case to Figure 8, also showing a transmigrated LL3 with evidence of cystic change.Figure 10. 3D and axial view of a CBCT scan showing the significant displacement of the LL2 caused by the transmigrated LR3.Figure 11. An OPG showing a transmigrated LR3 in close proximity to the LL2.
Surgical removal
Patients may choose to undertake surgical removal of the unerupted mandibular canine. Alternatively, the clinician may request its removal when orthodontic tooth movement is planned because leaving the tooth in position may limit alignment of the lower teeth.
However, many factors influence this decision:
Pre-existing pathology, including infection, cyst or a tumour relating to the unerupted canine
The degree of displacement of the mandibular canine (Figure 12)
Favourable long-term prognosis of the primary mandibular canine (Figure 13)
The existing malocclusion and amount of crowding present within the mandibular arch
Patient attitude to orthodontic treatment
Figure 12. Intra-oral photograph showing an LL3 that has erupted in the midline labial to the lower incisors.Figure 13. OPG showing a transmigrated LL3 and retained LLC with a fair long-term prognosis due to its relatively intact root.
If the decision is made for removal of the unerupted mandibular canine, and maintenance of a unilateral primary mandibular canine, a lower dental centre-line shift is often accepted due to the resultant tooth-size discrepancy (Figure 14).
Figure 14. Intra-oral photograph at debond showing non-coincidental dental centre lines due to the resultant tooth size discrepancy produced by retention of the LLC.
Exposure and orthodontic alignment
Although exposure and orthodontic alignment is the lengthiest in terms of treatment time, it can also produce the best functional and aesthetic results if undertaken successfully. This option is preferable in cases where resorption has already occurred to the roots of adjacent teeth or where the patient suffers from hypodontia, indicating preservation of teeth that are present.
The chosen method for surgical exposure varies depending on the position of the canine and the individual preference of the clinician, with evidence showing little difference in relation to treatment duration and periodontal health between the available techniques.13
Prior to this procedure, sufficient space to fully align the canine may be generated with fixed appliances and use of ‘push–pull’ mechanics. On occasions this may lead to spontaneous eruption of the impacted canine eliminating the need for surgical intervention (Figure 15).
Figure 15.
(a) OPG showing impacted UL3, LL3 and LR3. (b) OPG taken following space creation with fixed appliance treatment prior to expose and bonding both the LL3 and LR3. Fortunately, with space creation alone, the UL3 was able to successfully erupt without the requirement for surgical intervention.
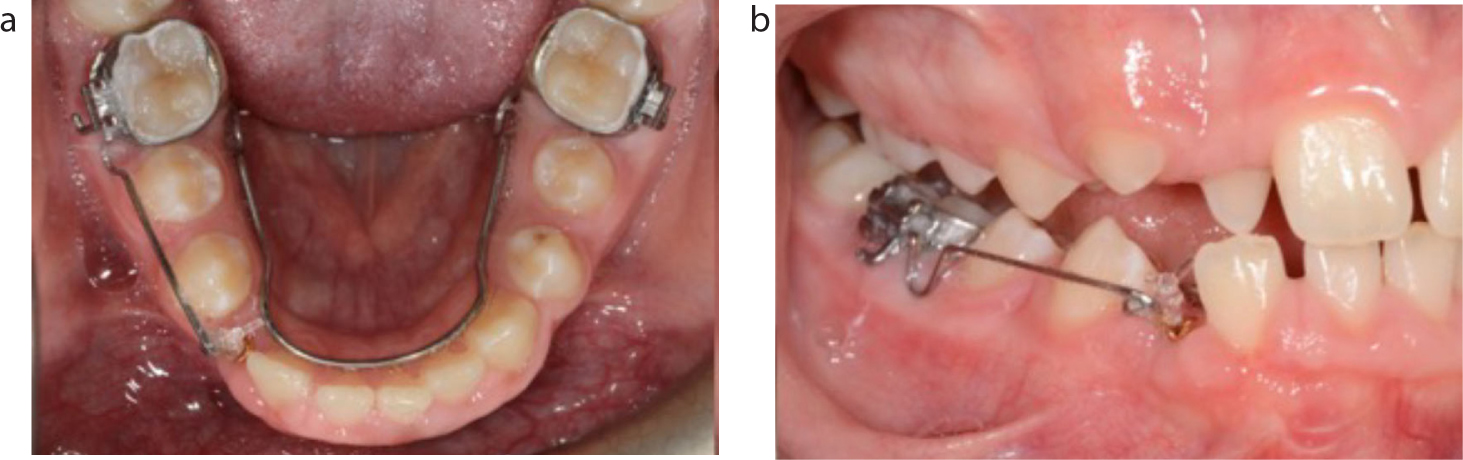
More than one technique is often used to mechanically erupt the canine. One of these methods involves use of a sectional cantilever fixed appliance (also known as a ‘fishing rod’) to initially guide eruption with the aid of a lingual arch to reinforce vertical anchorage (Figure 16).
Figure 16.
(a, b) Intra-oral photographs of orthodontic traction being applied to an impacted LR3 via a sectional cantilever fixed appliance (‘fishing rod’) with use of a lingual arch to reinforce vertical anchorage.
As further eruption of the tooth occurs, comprehensive fixed appliance treatment is often necessary to create sufficient space within the arch to accommodate the canine and to correct any overeruption from the opposing dentition (Figure 17).
Figure 17. Intra-oral photograph showing orthodontic traction being applied to a buccally impacted LL3 in a rigid lower 0.018-inch diameter base stainless steel archwire. Note how the opposing maxillary canine has overerupted.
The success rate of orthodontic traction to displaced teeth is reduced in older patients due to their reduced eruptive potential, therefore, identification of impaction at an early stage is important. In addition, the alignment of mandibular canines can often be more challenging and anchorage-demanding than that of maxillary canines owing to the greater relative mandibular bone density, especially around the anterior mandibular region.14 Modern advances in technology, such as the advent of temporary anchorage devices, have helped negate the effects of anchorage loss, resulting in outcomes that were previously not possible.15 However, there are still instances, in particular with transmigrated mandibular canines, where the unerupted teeth may be in highly unfavourable positions for orthodontic alignment.
Autotransplantation
Autotransplantation involves the surgical removal of the unerupted tooth and subsequent implantation into its normal position within the mandibular alveolus. Space will be needed in order to accommodate this tooth and will often be created prior to the operation with a short course of orthodontic treatment. Although this method has benefits, including a reduced treatment time compared with aligning the tooth with orthodontic traction, this method is very technique-sensitive and is rarely undertaken because studies have shown that autotransplanted teeth have poorer long-term prognosis owing to increased susceptibility to ankylosis and external root resorption.16 However, if successful, a transplanted canine in a child can provide a functional unit and preserve alveolar bone until definitive replacement with an implant-retained prosthesis is an option.
Conclusion
Unerupted mandibular canines can present with many variations, resulting in the management of this condition being heavily case-dependant. Successful correction of these teeth is important for both functional and aesthetic purposes. However, their management is complex and often requires input from a multidisciplinary team including both orthodontists and oral surgeons. Consequently, prompt identification and referral at an early stage is essential to reduce the risk of deleterious consequences and enable more predictable treatment outcomes.