Moher D, Liberati A, Tetzlaff J, Altman DG Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg. 2010; 8:336-441 https://doi.org/10.1016/j.ijsu.2010.02.007
Hoseini M, Mostafavi SM, Rezaei N, Boluri EJ. Orthodontic wire ingestion during treatment: reporting a case and review the management of foreign body ingestion or aspiration (emergencies). Case Rep Dent. 2013; 2013 https://doi.org/10.1155/2013/426591
Naragond A, Kenganal S, Rajasigamani K, Kumar NS. Accidental ingestion of molar band and its management: maintenance is better than management. Case Rep Dent. 2013; 2013 https://doi.org/10.1155/2013/891304
Shepherd T, Teo A, Naunton-Morgan R. Orthodontic braces come back to bite: a novel presentation of a small bowel volvulus. BMJ Case Rep. 2017; 2017 https://doi.org/10.1136/bcr-2017-221152
Jauhar P, Machesney MR, Sharma PK. Ingestion of an orthodontic archwire resulting in a perforated bowel: a case report. J Orthod. 2016; 43:237-240 https://doi.org/10.1080/14653125.2016.1201907
Tiller M, Schepp W, Gundling F, Tuerck J. Chronic pancreatitis caused by a swallowed orthodontic device. Endoscopy. 2014; 46:E667-668 https://doi.org/10.1055/s-0034-1390866
Monini Ada C, Maia LG, Jacob HB, Gandini LG Accidental swallowing of orthodontic expansion appliance key. Am J Orthod Dentofacial Orthop. 2011; 140:266-268 https://doi.org/10.1016/j.ajodo.2011.05.009
Al-Wahadni A, Al Hamad KQ, Al-Tarawneh A. Foreign body ingestion and aspiration in dentistry: a review of the literature and reports of three cases. Dent Update. 2006; 33:561-570 https://doi.org/10.12968/denu.2006.33.9.561
Umesan UK, Ahmad W, Balakrishnan P. Laryngeal impaction of an archwire segment after accidental ingestion during orthodontic adjustment. Am J Orthod Dentofacial Orthop. 2012; 142:264-268 https://doi.org/10.1016/j.ajodo.2011.05.025
Wilmott SE, Ikeagwuani O, McLeod NM. An orthodontic bracket embedded in the medial pterygoid surface: a case report. J Orthod. 2016; 43:65-67 https://doi.org/10.1179/1465313314Y.0000000113
Puryer J, McNamara C, Sandy J, Ireland T. an ingested orthodontic wire fragment: a case report. Dent J (Basel). 2016; 4 https://doi.org/10.3390/dj4030024
Booth-Mason S, Birnie D. Penetrating eye injury from orthodontic headgear – a case report. Eur J Orthod. 1988; 10:111-114 https://doi.org/10.1093/ejo/10.2.111
Zamir E, Hemo Y, Zauberman H. Traumatic Streptococcus viridans endophthalmitis after penetrating ocular injury from orthodontic headgear. J Pediatr Ophthalmol Strabismus. 1999; 36:224-225
Blum-Hareuveni T, Rehany U, Rumelt S. Devastating endophthalmitis following penetrating ocular injury during night sleep from orthodontic headgear: case report and literature review. Graefes Arch Clin Exp Ophthalmol. 2006; 244:253-258 https://doi.org/10.1007/s00417-005-1163-4
Conti G, Dolci M, Borgonovo A, Maiorana C. Aesthetic restoration of upper lip after removal of post-trauma foreign body (orthodontic bracket). Eur J Paediatr Dent. 2012; 13:239-240
Chandra RV, Anumala N, Vikrant V. An asymptomatic orthodontic bracket in the mandibular alveolar bone region. BMJ Case Rep. 2013; 2013 https://doi.org/10.1136/bcr-2013-009866
Samuels RH, Willner F, Knox J, Jones ML. A national survey of orthodontic facebow injuries in the UK and Eire. Br J Orthod. 1996; 23:11-20 https://doi.org/10.1179/bjo.23.1.11
Adverse outcomes of orthodontic treatment have been reported in the literature, yet there are currently no systematic reviews on the subject. We undertook a comprehensive review of the literature using the Medline and Ovid electronic databases, complemented by manual searching. The occurrence of unforeseen iatrogenic traumatic complications due to orthodontic treatment was used as the primary outcome. Traumatic iatrogenic complications associated with orthodontic treatment are infrequent. The most common complication reported is ingestion of orthodontic components. In the majority of the cases, management of the offending agent resulted in complete recovery without further complaint. The exception to this is ocular injury sustained as a result of improper use of or accidental injuries related to orthodontic headgear. These injuries are potentially devastating for the patient.
CPD/Clinical Relevance: Orthodontic treatment is carried out routinely and it is important to be aware of the unexpected complications that can occur during treatment and their consequences.
Article
Complications associated with orthodontic treatment are known, yet their occurrence cannot be completely eliminated. As these complications can adversely affect the patient–clinician relationship and prolong treatment time, every effort should be made to avoid them. In addition, discussion of potential unexpected outcomes of treatment is particularly important in view of the Montgomery ruling (Montgomery v Lanarkshire Health Board, 2015, SC 11.1AC 1430). Established in 2015, this ruling reinforced the importance of informed consent, material risk and recognizing patients as key decisionmakers.
Commonly discussed adverse outcomes of orthodontic treatment can be divided into those affecting hard tissue and soft tissue. These are summarized in Table 1.1
Hard tissue
Soft tissue
Dental cariesEnamel demineralizationRoot resorptionPulp damage and loss of vitalityTreatment failure in the form of relapse
Localized minor soft tissue injuryLocalized allergic reactionPeriodontal diseaseIatrogenic trauma related to temporary anchorage devices
Traumatic iatrogenic complications (TICs) in orthodontics are less frequent and less documented. TICs can either be caused due to incorrect use of the device(s) or following accidental injuries from the device(s). These can potentially lead to devastating outcomes for the patient.
There are currently no systematic reviews that assess these aforementioned TICs during orthodontic treatment.
Objective
The objective of this systematic review is to summarize the incidence of TICs following orthodontic treatment, with the primary outcome being complications caused during treatment, as a result of misuse of orthodontic devices or secondary accidental injuries.
Methods
A comprehensive review of the literature was conducted using the MEDLINE and Ovid electronic databases, complemented by manual searching of reference articles, from April 1940 to April 2018.
Two independent reviewers analysed the literature on the subject using the Covidence platform.
The search strategy included only terms relating to, or describing, traumatic injuries due to orthodontic treatment. The terms were combined with Cochrane MEDLINE filters. The search strategies employed for MEDLINE are available in Appendix 1.
Inclusion criteria included prospective and retrospective full-text cohort studies and case reports in English.
Exclusion criteria removed studies reporting on all the common complications of orthodontic treatment including: enamel demineralization, dental caries, root resorption, periodontal disease, treatment failure in the form of relapse, soft tissue trauma due to chemical, thermal or physical irritation, allergic reaction to components containing nickel, temporomandibular joint dysfunction secondary to orthodontic treatment and iatrogenic trauma related to temporary anchorage devices.
Results
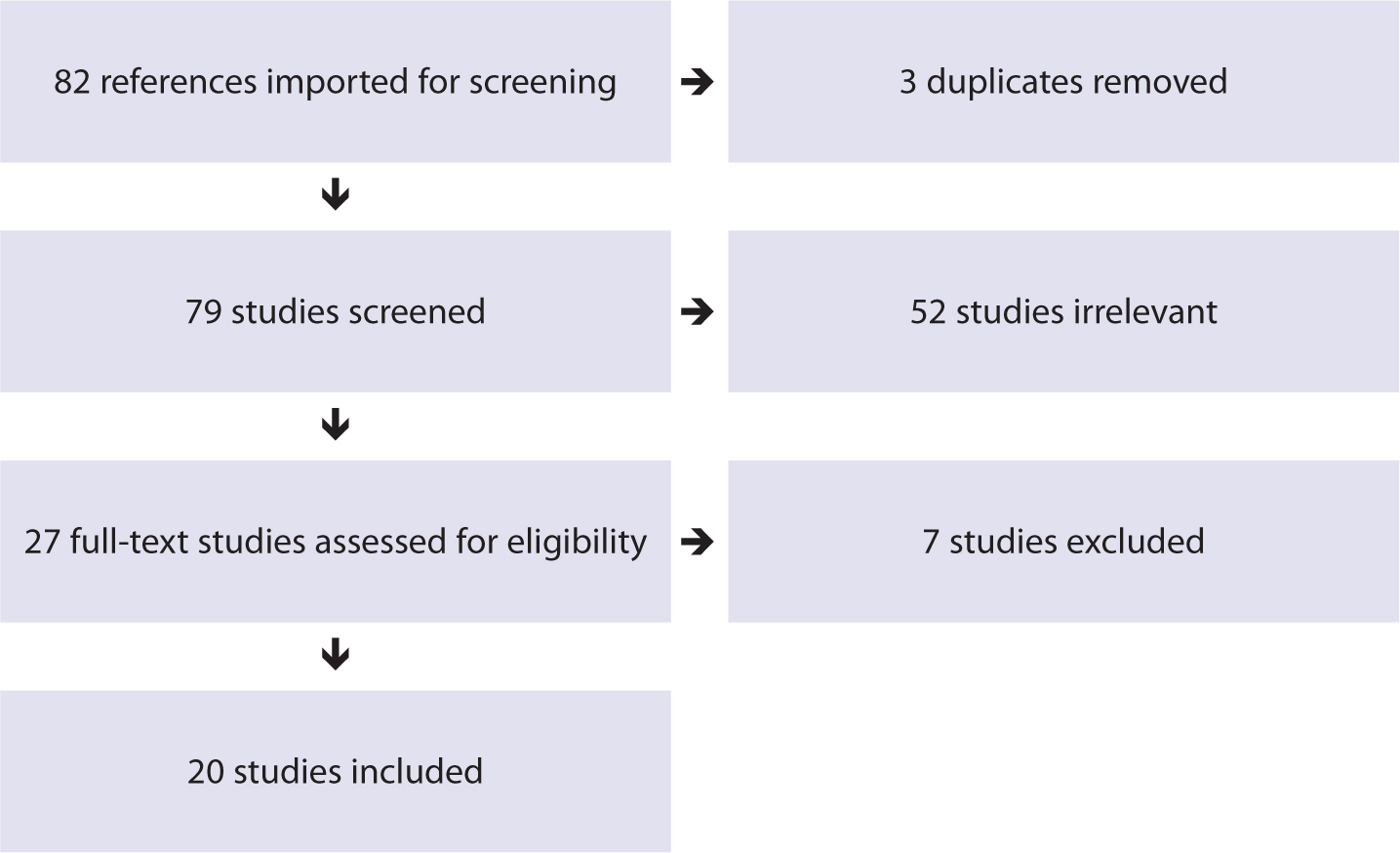
Figure 1 summarizes the selection process as per the PRISMA statement.2 In total, 20 eligible studies were included in this systematic review.
Figure 1. PRISMA flowchart outlining the results.
These 20 studies involved 21 patients: nine males and 12 females with an age range of 9–30 years. The details of the included studies are summarized in Table 2.
Presentation to emergency department with worsening central abdominal pain Perforation of small bowel by orthodontic wire Orthodontic treatment many years previously
Inhalation during treatmentThe fragment had then been naturally relocated and ingested
Inhalation of wire during treatment Wire found to be embedded in piriform recessAsymptomatic
Attempted endoscopic retrieval but wire could not be found on exploration of the piriform recess, larynx or oesophagusThe archwire fragment had relocated and had been ingestedConservative approach and wire had naturally passed through gastrointestinal tract
Inhalation/dislodgement of orthodontic bracket during routine adjustment of fixed orthodontic appliance
Symptoms of ‘scratchy’ throat and difficulty swallowing Area of firmness palpable over the mucosa anterior to her left tonsil. Bracket positioned in the medial pterygoid space
Delayed presentation 25 years after orthodontic treatment Presented with epigastric pain due to pancreatic duct dilatationChronic pancreatitis caused by obstruction of the papilla Vateri by an orthodontic device implanted years earlier
? bracket into extraction socket of lower left first premolar during procedure
Asymptomatic orthodontic bracket found in alveolar bone lower left premolar region on routine OPG Foreign body palpable but no inflammation/suppuration (delayed presentation)
Broken twin block appliance not reported by patient and continued useFollowing swallowing the broken fragment, the patient woke up breathless with a severe coughThe fragment became lodged in the oesophagus, which was later confirmed by endoscopy
Both eyes affectedRE: corneal laceration and prolapsed irisLE: limbal laceration and prolapsed iris
Medical and surgical management
RE: Phthisis and light perceptionLE: Reduced visual acuity
F/13
Orthodontic headgear
Dislocation while playing
Corneal abrasion
Medical and surgical management
Phthisis and light perception
F: female, M: male, OPG: orthopantomogram, RE: right eye, LE: left eye
The highest incidence of TICs reported were ingested orthodontic components (nine). Endoscopic retrieval of the components was required in three cases,3,4,5 while surgical management was the treatment in three cases.6,7,8 Conservative management and spontaneous passing of the component from the gastrointestinal tract (GIT) took place in the remaining three cases.9,10,11 The outcome in all reported cases was complete recovery without further complaint.
Inhalation of orthodontic components was reported in four cases: endoscopic retrieval,12,13 surgical removal14 and conservative management15 of the foreign body led to complete recovery without further complaint.
Ocular injuries were sustained as a result of orthodontic headgear misuse or accidental injury in six cases. These injuries resulted in endophthalmitis and subsequent loss of total vision in two cases,16,17 reduced vision to perception of hand movement in one case,18 along with phthitis with vision reduced to light perception or less in three cases.19,20
Two cases reported anatomical dislodgement of an orthodontic bracket. The brackets were dislodged in the upper lip21 and alveolar bone.22 In both cases the outcome was complete recovery without further complaint following retrieval of the embedded orthodontic bracket.
Discussion
Results of this systematic review show that TICs associated with orthodontic treatment are infrequent or under-reported. The most commonly reported complication is ingestion of an orthodontic component.
Foreign body aspiration or ingestion can pose a significant health risk for the affected individual. Dental objects are among the most widely reported objects to be aspirated or ingested.11 Depending on the size, shape and location of these objects, the outcome can vary.
Although less common, aspiration of dental objects can cause immediate respiratory distress or lead to long-term complications, such as infection, pneumonia, lung abscess oratelectasis.11
While the majority of ingested dental objectstend to pass through the GIT spontaneously, up to 20% may need to be removed endoscopically and 1% require surgery.11 Ingestion of sharp dental objects maylead to perforation, haemorrhage, impaction or even death.
In two reports, there was delayed presentation of the patient 10 and 25 years after orthodontic treatment. Both patients presented due to symptoms of worsening abdominal pain and following investigations, thediagnosis was perforation of the small bowelby an orthodontic wire6 and chronic pancreatitis caused by obstruction of the papilla Vateri by a Kobayashi ligature.8
Surgical management of both patients lead to complete resolution without further complaint.
In the remaining cases, once ingestion/inhalation of the offending agent was identified, steps were taken to localize the object by careful examination of the oral cavity and the oropharynx and once this failed, the patient was appropriately taken to the emergency room immediately. Following investigations and localizing the object, either a conservative approach was taken to monitor the natural passing through the GIT or alternatively the object was endoscopically removed.
The British Orthodontic Society provides guidance on management of inhaled/ingested orthodontic components and outlines a systematic plan of action.23, In all of the cases included in this review, with the exception of the delayed presentations, this protocol was followed appropriately and thus the outcome was complete recovery without further complaint.
The TIC associated with the most devastating outcome is ocular injury sustained as a result of improper use or accidental disengagement of components of headgear where there is potential for considerable ocular trauma.
This is thought to be due to the design of the intra-oral bow that could cause bilateral penetrating ocular injury as the distance between the two ends of the bow is very similar to the inter-pupillary distance. Furthermore, inoculation of the oral microflora into the eye can lead to overwhelming infection and subsequent loss of vision.24
From review of the literature, it would appear that reports of these injuries have appeared since the 1970s. Several guidelines have since been established in order to ensure safety features are incorporated into the headgear design. These include safety release or snap-away headcaps/neck straps, as well as locking facebows. On review of the current literature, it would appear that these safety mechanisms are not completely sufficient to eliminate the occurrence of injuries as they still leave room for disengagement of components, especially during the night.
A survey of 1117 practitioners in the UK reported that, of the practitioners who reported an injury, 93% of their patients experienced detachment at night and the majority of the injuries (71%) were found to occur at night.25
Conversely, the most recent cases of ocular injury were related to orthodontic headgear without safety mechanisms,18 as was the case prior to this.20 Safety mechanisms have improved since then.
This review highlights the continual need for improvement of the safety features of headgear as well as establishment or improvement of current guidelines on correct use of headgear.
Conclusion
TICs associated with orthodontic treatment have continued to appear in the literature for the past 40 years. This is despite establishment of guidance regarding safety features of orthodontic devices. The reported causes of these injuries include incorrect use of the device, accidental disengagement, inhalation or ingestion of the components.
Ingestion of orthodontic components appears to be the most commonly reported TIC associated with orthodontic treatments based on the literature, while ocular injuries related to orthodontic headgear have the most devastating outcome.
Patients must be made aware of the devastating potential consequence of incorrect use of orthodontic headgear. This review highlights the need for improvement of the current guidelines or establishment of new guidelines.