Thorstenson GA, Kusy RP. Resistance to sliding of self-ligating brackets versus conventional stainless steel twin brackets with second-order angulation in the dry and wet (saliva) states. Am J Orthod Dentofac Orthoped. 2001; 120:361-370
Henao SP, Kusy RP. Evaluation of the frictional resistance of conventional and self-ligating bracket designs using standardized archwires and dental typodonts. Angle Orthod. 2004; 74:202-211
Shivapuja PK, Berger J. A comparative study of conventional ligation and self-ligation bracket systems. Am J Orthod Dentofac Orthoped. 1994; 106:472-480
Rossouw EP. Friction: an overview. Semin Orthod. 2003; 9:218-222
Kusy RP. Ongoing innovations in biomechanics and materials for the new millennium. Angle Orthod. 2000; 70:366-376
Forsberg CM, Brattström V, Malmberg E, Nord CE. Ligature wires and elastomeric rings: two methods of ligation, and their association with microbial colonization of Streptococcus mutans and lactobacilli. Eur J Orthod. 1991; 13:416-420
McLaughlin RP, Bennett JC. The transition from standard edgewise to preadjusted appliance systems. J Clin Orthod. 1989; 23:142-153
Irvine R, Power S, McDonald F. The effectiveness of laceback ligatures: a randomized controlled clinical trial. J Orthod. 2004; 31:303-311
Usmani T, O'Brien KD, Worthington HV, Derwent S, Fox D, Harrison S A randomized clinical trial to compare the effectiveness of canine lacebacks with reference to canine tip. J Orthod. 2002; 29:281-286
Fleming PS, Johal A, Pandis N. The effectiveness of laceback ligatures during initial orthodontic alignment: a systematic review and meta-analysis. Eur J Orthod. 2012;
Halimi A, Benyahia H, Doukkali A, Azeroual MF, Zaoui F. A systematic review of force decay in orthodontic elastomeric power chains. Int Orthod. 2012; 10:223-240
Elhussein MA, Sandler PJ. Effective Derotation of canines and premolars. J Clin Orthod. 2016; 50
Using stainless steel auxiliary ligatures in conjunction with fixed orthodontic appliances is of paramount importance in many stages of orthodontic treatment. There is a lack of articles in the literature that provides a comprehensive review of the uses of different methods of ligation in orthodontic treatment. The aim of this article is to provide an illustrated review of their use with fixed appliances; moreover, it will provide practical tips for their appropriate use.
CPD/Clinical Relevance: This article aims to provide a review, with detailed illustration, of the use of stainless steel ligatures in orthodontic treatment.
Article
Orthodontic techniques have evolved significantly over the past three decades. The use of stainless steel auxiliary ligatures with fixed orthodontic appliances contributes significantly to the efficiency and the effectiveness of tooth movement, largely due to the so-called frictionless or low-friction mechanics,1,2,3 much more effective engagement of the archwire into the bracket slot and the advantage of being a much less plaque retentivearrangement.4,5
Elastomeric modules are by far the most popular method of ligation of archwires; they are preformed, convenient and allow rapid archwire engagement, yet they have disadvantages: mainly saliva/bacteria absorption causing reduced effectiveness with time, and limited elastic properties that sometimes compromise full archwireengagement.6
The uses of stainless steel ligatures with fixed appliances include the following:
Lacebacks
Continuous ligature ‘pigtail’
Dead ligatures
Figure of eight ‘underties’
Short stainless steel ligatures/quick ligs
Figure of eight Kobayashi ties.
Lacebacks
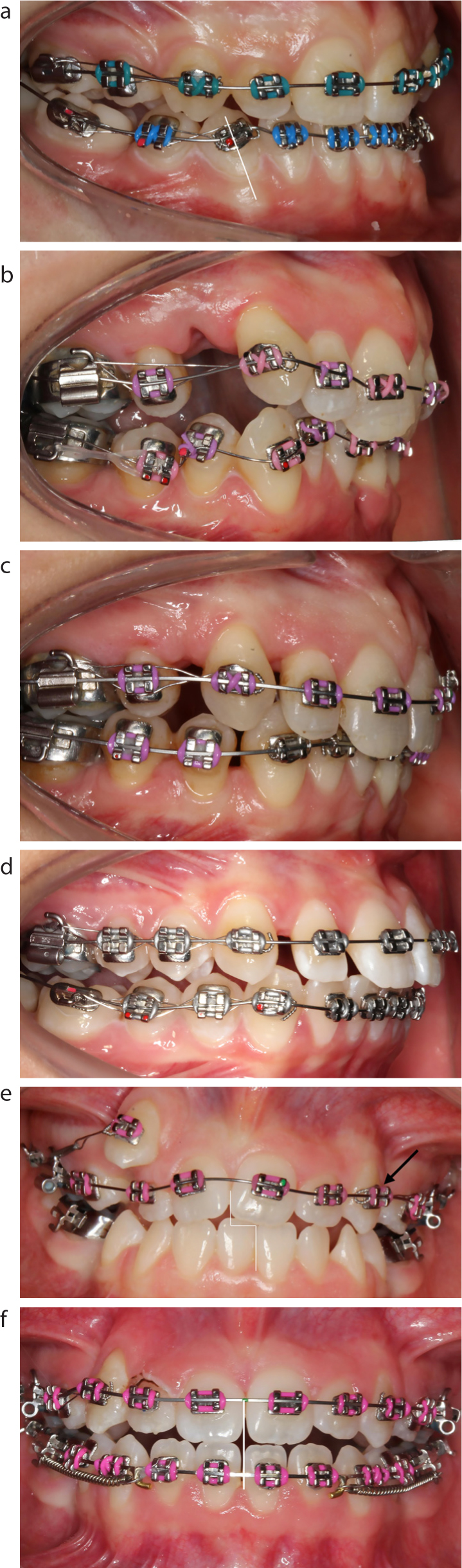
The use of lacebacks in orthodontic clinical practice constitutes an area of controversy both among clinicians and in the literature. Lacebacks were primarily popularized by McLaughlin and Bennett as part of the MBT system.7 A laceback is typically placed passively underneath an archwire in a figure of eight pattern, from the first molar hook to the mesial of a canine bracket. Lacebacks are used with upright or distally inclined canines (Figure 1a) and are intended to fix the molar–canine distance, thus preventing the tip built into the canine brackets being expressed by forward canine crown displacement during the levelling and aligning phase, and proclination of the incisors. Because the distance is fixed, the only way that the archwire can level, and thus the canine crown can align, is by the root of the canine moving in a distal direction, which in most cases is usually the most desirable movement. In crowded cases, where space has been created by extraction of premolar units, canines may also be gently retracted as a result of the forces of mastication onto the sections of laceback between the teeth (Figure 1b,c).
Figure 1. (a) Laceback in the lower right quadrant prevents the LR3 crown mesializing. (b) Laceback encourages mesialization of UR5 and UR6, whilst the UR3 is being retracted. (c) In only 12 weeks, UR3 is in a Class I relationship and UR6 is in a Class II relationship. (d) Laceback placed to limit lower incisor proclination. (e) Laceback placed to encourage the upper centreline movement to the left and (f) 6 months later, centreline correction achieved.
The tip in the canine bracket might place a strain on posterior anchorage,8 hence, leading to anchorage loss by mesial movement of posterior teeth. If that is an undesirable movement, anchorage supplementation will need to be employed. Mesial molar movement, however, is often desirable during treatment, therefore the use of a laceback can be considered an efficient and effective way in achieving this.
There is a lack of quality scientific evidence available in the literature either supporting or refuting laceback use, so, in the absence of persuasive evidence either way, it ends up being a matter of personal preference of the operator. It therefore rests with the orthodontist to assess the quality of clinical results they encounter, achieved both with and without laceback use, to enable them to decide how they wish to practise clinically.
Lacebacks are manufactured from soft grade stainless steel and a popular size is 0.009” preformed ligature wire. They are most commonly prescribed to:
Limit incisor proclination during alignment; by controlling mesial tip of canines during levelling and aligning (Figure 1d);9,10
Actively retract canines and mesialize molars during levelling and aligning in extraction cases;10
Fix the distance between molar and canine teeth where this would be beneficial;
Aid dental centreline correction, by applying unilaterally;
Protect spans of unsupported wire in the early stages of alignment, particularly when light nickel–titanium wires are used (Figure 1e,f).
Long stainless steel ligatures
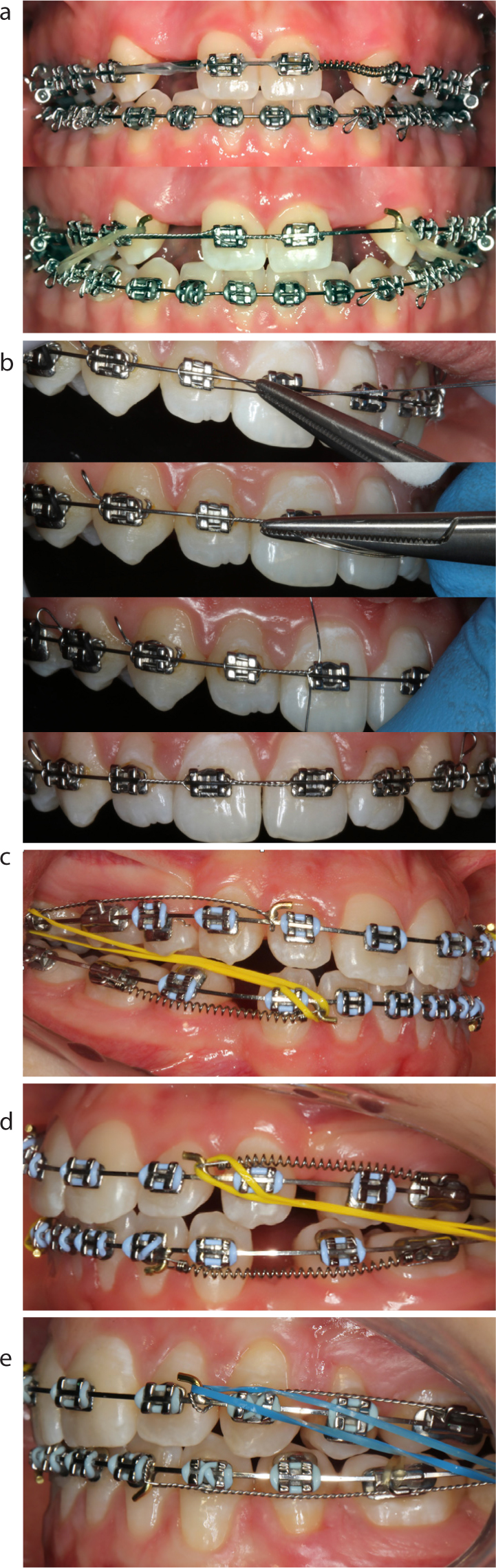
In complex orthodontic cases, such as in the treatment of hypodontia, space redistribution and space closure is a phase that can present significant challenges. It is important that orthodontically closed spaces remain closed, and that spaces that have been created remain open, with no diminution or increase in their size with time, until treatment moves seamlessly into the retention phase (Figure 2a,b). A ‘continuous ligature’ can also be used to the soldered post or crimped hook on an archwire, when unilateral space closure is being effected, to prevent the archwire from just sliding towards the contralateral side, as a result of space closing mechanics. This will also maintain dental centreline symmetry (Figure 2c,d). Placement of a continuous pigtail stainless steel ligature (dead ligature) is also highly recommended when premolar extraction spaces are closed because it prevents the slight space, often seen in the buccal segments, from reopening (Figure 2e).
Figure 2. (a) Redistribution of anterior spaces, maintained with a continuous ligature. (b) Technique of placement of a continuous ‘pigtail’ ligature. (c, d) Continuous ligature to hook to prevent archwire from sliding while space closure proceeding on the left. (e) Dead ligatures placed to prevent premolar space reopening.
Figure of eight tie
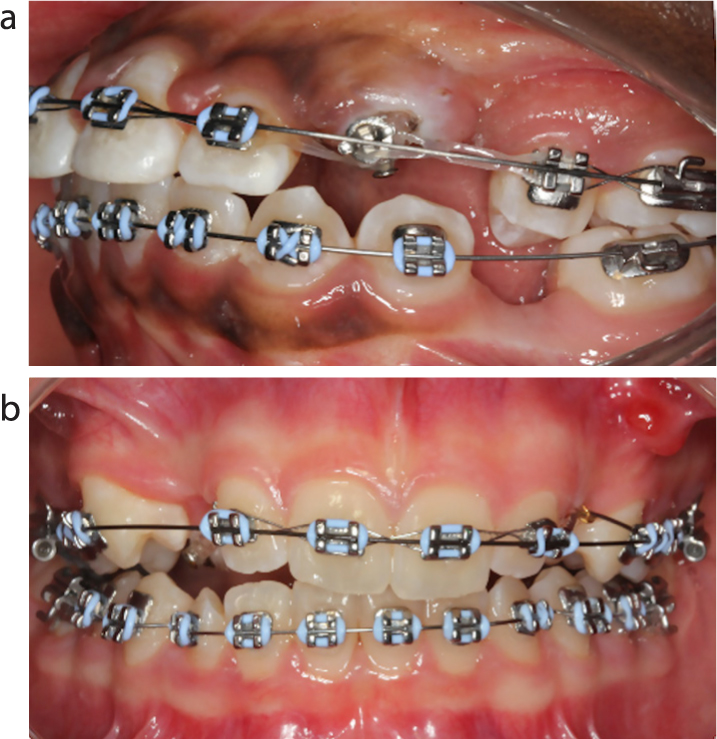
An undertie is a modification of a laceback, normally placed to reinforce anchorage by ligating a number of teeth as a block. It can be used in many different ways depending on the desired tooth movement, for example, a figure of eight ligature from the molar hook to the mesial of a premolar bracket instead of a canine bracket (Figure 3a). The figure of eight is sometimes placed anteriorly just around incisor teeth (Figure 3b), but can be extended further posteriorly to increase the number of teeth in the anchorage unit as necessary. A disadvantage of the undertie is that the patient's tooth-cleaning ability is somewhat compromised because of the crossover of wire in the interdental spaces. A continuous ligature, which directly overlaps the archwire, is certainly a much cleaner and more precise alternative, although slightly more time-consuming to place.
Figure 3. (a) Underties placed anteriorly to increase the anchorage unit. (b) Modified laceback ‘undertie’ placed anteriorly to increase the anchorage unit.
Short stainless steel ligatures/quickligs
Conventionally, elastomeric modules are used to ligate archwires due to their ease of use and the choice of different colours, which has certainly made the use of fixed appliances more acceptable in children and adolescent patients. They usually undergo a rapid phase of force decay in the oral environment that necessitates their replacement at every fixed appliance adjustment.11 Furthermore, the rapid force decay renders them less effective when firm ligation is required at the bracket–wire interface. Short stainless steel ligatures manufactured from a 0.009” stainless steel ligature wire, can provide much more secure ligation at the archwire–bracket interface (Figure 4a,b).
Figure 4. (a,b) Technique for a short ‘quick tie’ stainless steel ligature. (c) Short stainless steel ligatures – cleanest and most efficient space closure technique. (d) Stainless steel ligatures prevent Ni–Ti coil rotating LL1 and LL3. (e) Ligated UR2 and UL2 prevents rotation while a powerchain is being used. (f)Steel ligature tied to derotate LL3.
Short stainless steel ligatures, when applied correctly, secure the archwire–bracket interface perfectly, and enhance sliding mechanics by reducing friction (Figure 4c), thus reducing the strain on anchorage. They offer a method of ligation that prevents any rotation of the teeth adjacent to active push coil (Figure 4d) or rotation of the terminal tooth in a length of powerchain (Figure 4e), so should, therefore, prevent the need for ‘round tipping’. It takes only a week or two to lose control and allow rotation of vulnerable teeth, but it will take 2–3months to regain control; therefore, it is advisable to spend a few more seconds placing stainless steel ligatures on these teeth. Moreover, stainless steel ligatures can be used during alignment when a light archwire is engaged into the bracket slot of a rotated tooth, as they are efficient enough to allow an effective force to be generated to derotate teeth (Figure 4f).12
Another advantage over elastomeric modules and powerchains is that they are infinitely cleaner and more hygienic, thus allowing longer intervals between appointments for appliance adjustments, if this is considered appropriate.
Summary of advantages of stainless steel ligatures over elastomeric ligation
Less plaque and saliva retention, morehygienic
Firm archwire ligation at the bracket–wire interface
More effective derotation of rotated teeth
Longer interval between appointments possible
Kobayashi ligature tie hooks
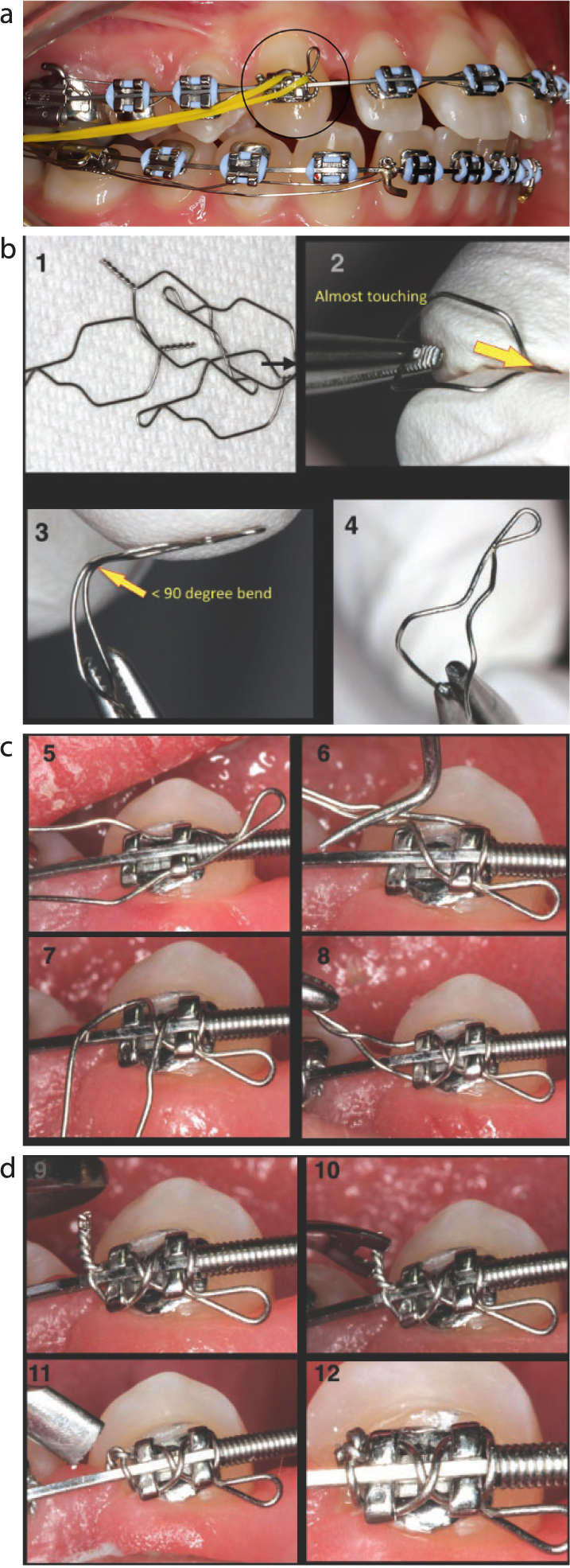
Kobayashi ties are easy to use with fixed appliances, often as a substitute for wire ligation as they serve both as an effective metal ligature and as a hook; excellent for attachments for intra-oral elastics (Figure 5a). They are manufactured from high-grade (hard) stainless steel with a dimension of 0.012”. The loop in the stainless steel ligature wire is spot-welded to form a hook. One frequently encountered problem in practice, is rotation of the hook when just tied around the four bracket wings, and patients often present as an orthodontic emergency due to a loose, rotating or missing Kobayashi tie. A useful ‘figure of eight’ modification is illustrated to securely ligate a Kobayashi hook, which allows for orthodontic mechanics to be optimized by efficient and trouble-free Kobayashi/elastic use (Figure 5b–d).
Figure 5. (a) Kobayashi tie placed to the UR3. (b,c) ‘Figure of eight’ technique, for firmly ligating Kobayashi ties. (d) Ligature tucker and oval amalgam packer indispensable to effectively manage pigtails, preventing trauma and facilitating oral hygiene.
Conclusions
There are many situations in which use of stainless steel auxiliary ligatures will significantly speed up orthodontic treatment by preventing unwanted side-effects. Appropriate use of stainless steel ligatures and effective deployment of both a ligature tucker and an oval amalgam packer is thought to be indispensable to prevent trauma, facilitate oral hygiene, maximize patient comfort and complete treatment in the shortest possible time. It is worth every clinician learning when and how to effectively use stainless steel ligatures to maximize the benefits for all of their patients.