This case report describes the diagnosis and treatment of a non-syndromic unilateral geminated second premolar complicated by hypodontia of three second premolars. Gemination is defined as a developmental disturbance of the shape of teeth and is usually recognized as a partial cleavage of a single tooth germ resulting in one root and one pulp space with two partially or totally separated crowns. Hypodontia is defined as the developmental absence of one or more teeth, excluding the third molars. Geminations of maxillary second premolars are rarely reported. These dental anomalies can cause local malocclusion manifesting as crowding or spacing.
CPD/Clinical Relevance: Diagnosis of dental anomalies such as gemination can be difficult. This paper discusses the diagnosis and management of one such case which involved CBCT.
Article
Paula Sinnott
Gemination is defined as a developmental disturbance of the shape of teeth and is usually recognized as a partial cleavage of a single tooth germ resulting in one root and one pulp space with two partially or totally separated crowns.1 Although it occurs in both dentitions, it has a higher occurrence in the primary dentition, especially in the anterior maxillary region. Unilateral gemination has a prevalence rate of 0.5% and 0.1% in deciduous and permanent dentition, respectively.2 Fusion normally results in one less tooth in the arch, however, an exception to this is the fusion between a supernumerary tooth and a tooth of the normal dental series. Management options of geminated teeth include accepting and monitoring, complex endodontics, or extraction.
Hypodontia is defined as the developmental absence of one or more teeth, excluding the third molars.3 The prevalence of hypodontia in the permanent dentition is estimated to be 6·4% in the UK.4 The aetiology of the condition is multifactorial and can be divided into genetic factors, environmental factors and/or systemic factors.5,6 The most commonly affected teeth are mandibular second premolars, followed by maxillary lateral incisors, maxillary second premolars and mandibular incisors.7,8
Management of hypodontia often requires close interdisciplinary treatment with contributions from the orthodontic, paediatric and restorative dentistry teams. There are several treatment options to manage spacing caused by hypodontia, depending on severity of hypodontia. In the majority of patients, orthodontic treatment will be required before this space can be restored satisfactorily; sometimes orthodontics can eliminate the need for restorative tooth replacement.9,10
This case report describes diagnosis and treatment of a non-syndromic unilateral geminated second premolar complicated by hypodontia of three second premolars. A literature review of gemination found very few reports.11,12,13,14,15 This anomaly is most common in primary maxillary incisors. Gemination of maxillary central incisors and molars with supernumerary teeth were reported by many authors, whereas geminations of maxillary second premolars are rarely reported. This dental anomaly can cause local malocclusion manifesting as crowding or spacing.
Case report
A 14-year-old fit and healthy male was referred to the Orthodontic Department by a primary care specialist in Orthodontics for the removal of an impacted supernumerary in the upper right second premolar region. The patient was seen on a multidisciplinary clinic involving specialists in Orthodontics and Oral Surgery.
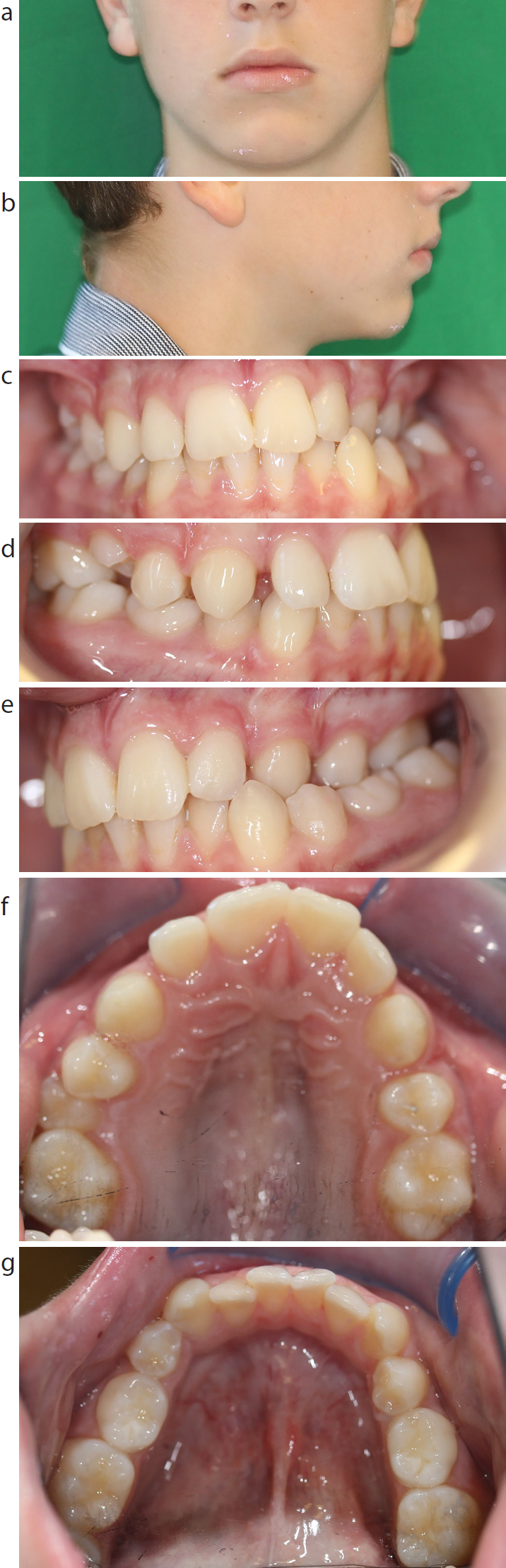
He presented with a Class I incisor relationship on a Class I skeletal base, with average vertical facial proportions. There was no facial asymmetry noted. The malocclusion was further complicated by developmental absence of the upper left second and lower second premolars. The lower deciduous second molars were retained. The upper right second premolar was partially erupted and rotated mesiopalatally. There was mild crowding in the lower arch and spacing in the upper arch, except in the area of the upper right second premolar. A left unilateral buccal crossbite involving the upper left canine, first premolar and first molar, without displacement, was present. There was a Class I molar relationship bilaterally and quarter unit Class III canine relationship (Figure 1). The unerupted tooth was palpable buccal to the upper right second premolar in the first quadrant (Figure 2).
Figure 1.
(a–g) Pre-treatment extra-oral and intra-oral views: (a) extra-oral portrait; (b) lateral view; (c) frontal intra-oral; (d) right intra-oral; (e) left intra-oral; (f) maxillary occlusal; (g) mandibular occlusal.Figure 2. Intra-oral clinical examination revealed a partially erupted upper right second premolar which was rotated mesially.
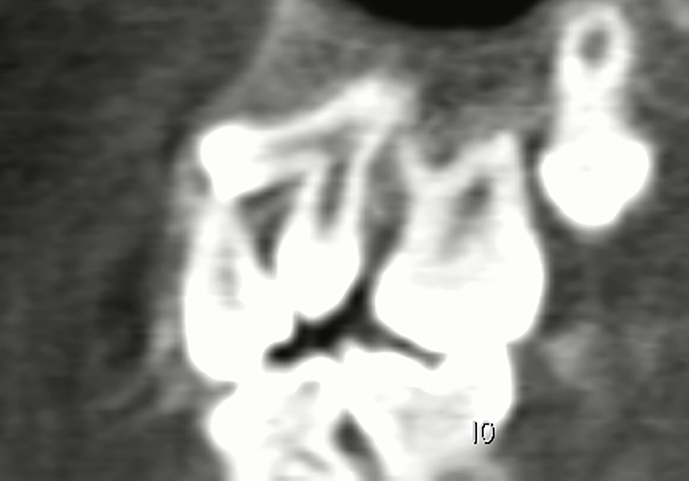
The orthopantogram confirmed developmental absence of the upper left second premolar and lower second premolars (Figure 3). A cone beam computed tomography (CBCT) was taken within primary care and included in the referral. The CBCT DICOM data (i-CAT scan) showed that, at almost right angles to the midpoint of the root of the upper right premolar, there was an additional dental structure with partial root and diminutive crown. The crown perforated the buccal cortical plate and the pulps were merged in the middle third of the root. There was a single root apex. The pulp of the two teeth was conjoined indicating gemination (Figure 4).
Figure 3. Orthopantogram showing hypodontia of the second premolars in all quadrants except the upper right quadrant and retained deciduous lower second molars.Figure 4. Cross-sections of the CBCT were able to reveal the intra-osseous location and morphology clearly, particularly the conjoined root canals of the geminated tooth, allowing accurate diagnosis.
Treatment plan
As the two dental structures were conjoined, it was not possible to undertake the request of the referrer to extract only the supernumerary in the upper right second premolar region. Due to the developmental absence of the other remaining second premolars, the presence of mild crowding and Class III canine tendency, the decision was made for the surgical removal of the upper right geminated second premolar along with the retained lower second deciduous molars. Upper and lower fixed appliances would then be provided to level and align the arches, close the residual spaces, treating to a Class I incisor, canine and molar relationship.
Treatment
The patient attended Pinderfields General Hospital for the surgical removal of the geminated upper right second premolar, along with the retained lower second deciduous molars, under general anaesthesia. The tooth morphology of the geminated tooth was examined (Figure 5) and showed fused roots with a bifid crown (Figure 6). The patient has been discharged from the Oral and Facial department for continuation of his orthodontic treatment with a specialist in Orthodontics within primary care.
Figure 5. Morphology of the geminated upper right second premolar post extraction.Figure 6. Surgical flap was lifted revealing bifid crown.
Discussion
Gemination and fusion are anomalies in size, shape and structure of teeth. Gemination results in either a large tooth with a bifid crown or two completely divided teeth throughout the crown and root. However, in fusion there is a single crown with typically two roots or a single root with two canals. The prevalence of gemination or fusion is 0.05% in the permanent dentition.16 Fusion normally results in one less tooth in the arch, however, an exception to this is when fusion is between a supernumerary tooth and a normal tooth of the dental series.17 The CBCT scan in this case (Figure 4) shows that the pulp of the two teeth is conjoined, confirming gemination rather than fusion.
The aetiology of gemination is still unclear. There appears to be a genetic component and it often appears with hypodontia, as illustrated in this case. Anomalies of number, size and shape seen together clinically in the same dentition are due to processes during initiation and morphogenesis. The main aetiology of gemination remains unknown, but physical pressures leading to the union of teeth and genetic inheritance have been suggested as possible causes. Grover and Lorton claim that local metabolic interferences, which occur during morphodifferentiation of the tooth germ, may be the cause.15 They suggest that there could be a relationship amongst gemination, twinning and odontoma, while Lyroudia et al suggested trauma could be another possibility.18
Genetics, the environment and developmental timing are all believed to be aetiological factors which play a role in the development of hypodontia.19 Hypodontia may be associated with a syndrome or may exist in isolation. Cobourne described the role of homeobox genes and their link to hypodontia, with specific genes responsible for specific missing teeth.20 Mutations in MSX1, PAX9, AXIN2 and EDA have been identified in families with non-syndromic hypodontia.21 Other studies have described the importance of MSX1, MSX2 and muscle specific homeobox genes in dental development.6 Environmental factors linked to hypodontia include infection, drugs such as thalidomide, trauma and irradiation.22 A systemic illness at the time of tooth formation may also disturb specific tooth development. Although more recent studies focus on genetic factors, the multifactorial nature of this condition must be considered.
Radiographic assessment is mandatory in order to identify and treat appropriately the complexity of gemination/fusion. In cases of severe overlapping and superimposition of impacted teeth, it may not be possible to determine the accurate location of the teeth relative to surrounding structures using conventional two-dimensional radiographs.17 Traditionally, periapical, occlusal, and panoramic radiographs have been used to make these determinations. However, in some cases, it is difficult to determine the exact buccolingual relationships of teeth and surrounding structures using these views alone. On some periapical and occlusal radiographs, assessments of the facial or lingual position of dental anomalies are possible using a tube-shift (parallax) technique. In others, a true occlusal (cross-sectional) view may provide this information. Although conventional radiographs are usually able to provide sufficient detail, they fail to provide definitive information concerning the 3-dimensional relationship of the dental anomalies and the surrounding structures for surgical planning.23 In this case, a CBCT was able to reveal the intra-osseous location and morphology clearly, particularly the conjoined root canals of the geminated tooth, as well as its proximity to the adjacent teeth, sinus and cortical bone (Figure 4). This case illustrates the role of the CBCT scan in accurately diagnosing the dental anomaly and appropriately planning and treating this case. As clinicians we have a responsibility to deliver this technology to patients in a responsible way, so that diagnostic value is maximized and radiation doses are kept as low as reasonably practicable. CBCT radiographs, like any radiograph, must be justified on an individual basis by demonstrating that benefits outweigh the risks, especially for paediatric uses.24 CBCTs should add new information to aid patient management and be used for careful evaluation and treatment planning, as illustrated in this patient's case. A record of the justification process must be kept. When referring a patient for a CBCT examination, the referring clinician must supply sufficient clinical information (patient history and results of examination) to allow the CBCT practitioner to perform the ‘justification process’.24 It seems likely that CBCTs may have a role in pre-surgical assessment of any unerupted tooth where conventional radiographs fail to give the information required. Despite the expected advantage of CBCT in tooth localization, it is important to consider the impact upon management of patients, the increased radiation dose and the likely higher cost of CBCT examinations. When health professionals change their practice to adopt a more expensive diagnostic technique, particularly where there are radiation-related risks in a predominantly young patient age group, the onus is on them to demonstrate significant improvement in patient outcomes. According to the European Commission, the smallest volume size compatible with the situation should be selected because of reduced radiation dose.24
General management
Treatment options for geminated teeth include:
Doing nothing;
Accept and align;
Reduction in size;
Extraction and surgical hemi-section, depending on patient preference, site and features of geminated tooth, and the different aspects of the malocclusion.
Treatment plans regarding such dental anomalies often require specialist opinion.
In this case, the first option would be to do nothing or accept and monitor. Management of these dental anomalies may entail accepting the condition with regular review of the patient to prevent any complications, where aesthetics and function are acceptable. The second option is endodontic management. This option is dependent on the point of fusion, morphology of canals and then sectioning the geminated tooth. If this tooth was fused it may have been amenable to sectioning and subsequent root treatment. However, it was not fused, therefore this was not a viable option. The third option would be extraction of the geminated tooth, facilitating correction of any resultant malocclusion and closure of residual space. Following extraction, the options are either to close the space or open the space. One option would be to restore the space following extraction. This could be with an implant (when the patient is over 18 years of age), bridge or partial denture. However, in this case it was agreed with the patient and his parents to close the spaces after carrying out extraction of the geminated tooth and balancing extractions of the lower retained primary second molars to maintain symmetry and achieve Class I occlusion with the use of fixed appliances.