Effective multidisciplinary approach for treatment of traumatized maxillary incisors and hypodontia Jonathan J O'Dwyer Jonathan Sandler Dental Update 2024 13:1, 707-709.
Fractured and missing teeth within the aesthetic zone have always posed a clinical challenge for the dental team. Management and treatment requires the input from a number of dental specialists to guarantee a high quality result. A case report is presented to demonstrate an effective combined orthodontic/restorative approach that fully restored aesthetics and function. The report is of a 14-year-old girl who traumatized her maxillary central incisors, in a dentition that was already compromised as she had congenital absence of her maxillary left lateral incisor.
Using fixed orthodontic appliances, the fractured teeth were extruded to bring the fracture line above the level of the alveolar bone. This movement allowed an immediate aesthetic improvement, using stainless steel prefabricated posts and composite resin buildups, which also facilitated further orthodontic tooth movement. Teeth, that would otherwise have been extracted, were salvaged and, utilizing a multidisciplinary team approach, a reasonable long-term prognosis has resulted.
CPD/Clinical Relevance: This case report aims to demonstrate how a multidisciplinary team approach in Orthodontics can be utilized for management of severely handicapped dentitions that have sustained dental injury. It is not the aim of this case report to discuss the treatment of dental injuries but to demonstrate and provide an overview of the possible treatment modalities that can be effective in restoring function and aesthetics, with special consideration given to missing teeth and subgingival crown fractures within the aesthetic zone.
Article
Mustafa Elhussein
Trauma to the oral region occurs frequently and comprises 5% of all injuries for which people seek treatment.1 The incidence of traumatic dental injury is common, with between 6%–34% of children aged 8-15 years experiencing damage to their permanent teeth.2,3,4 Hypodontia is often defined as the developmental absence of one or more primary or secondary teeth, excluding third permanent molars,5 and is a relatively common condition affecting around 4% of the British population.6 Due to the fact that an increased proportion of children who have sustained dental trauma seek orthodontic treatment, orthodontists need to be aware of the long-term prognosis of traumatized teeth and the implications on orthodontic treatment planning.
Case report
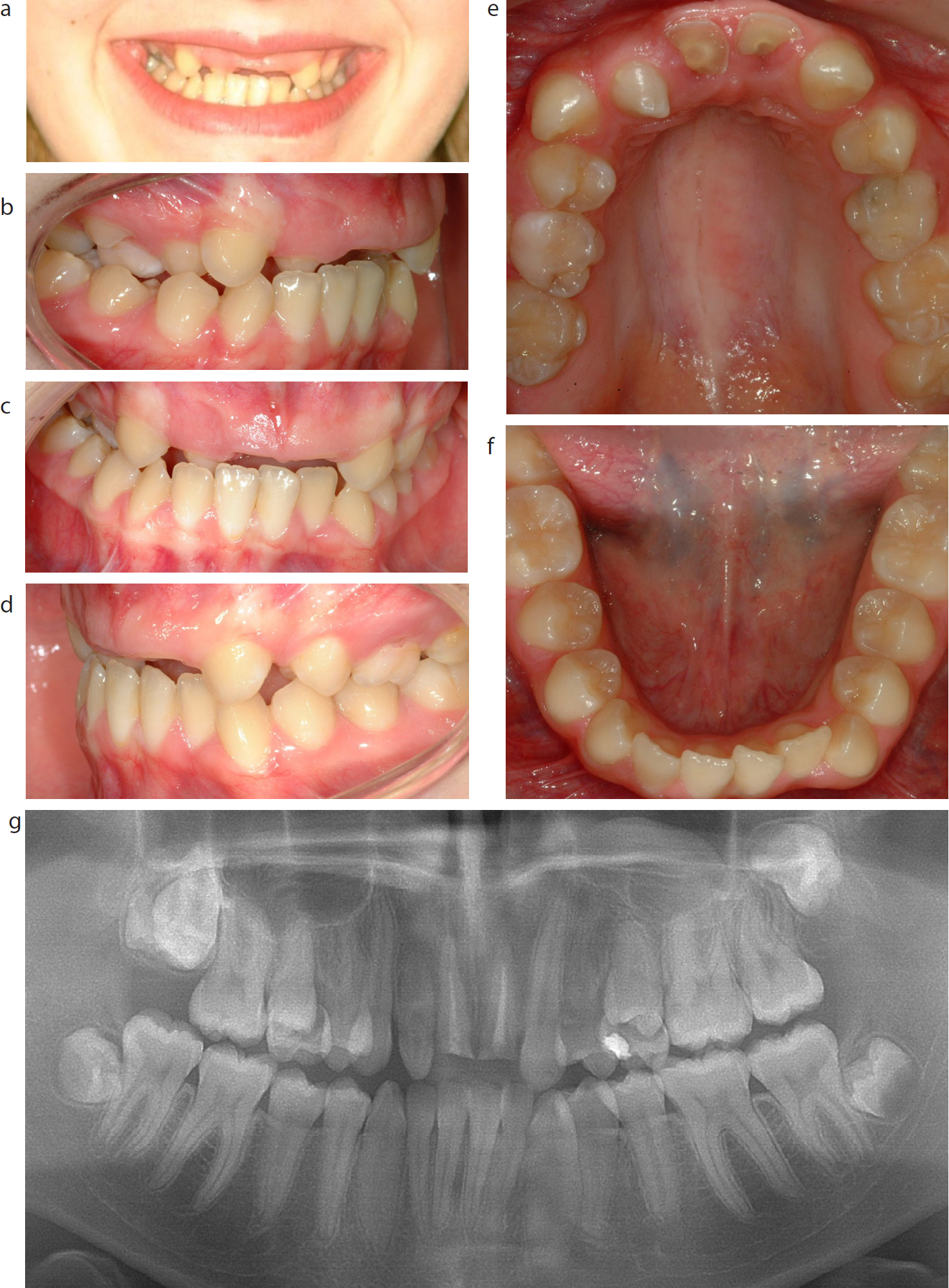
A 14-year-old girl was referred to the orthodontic department presenting with a history of trauma to both maxillary permanent central incisors. She had recently been accidentally hit in the face with a golf club. Her main complaint was the grossly unaesthetic appearance of her upper front teeth (Figure 1). The patient had a symmetrical face with an average lip line, a Class II profile and an average Frankfort-mandibular planes angle. Intra-oral examination revealed the presence of fractured maxillary central incisors and the remaining roots had been incompletely root filled (Figures 1, 3a). The situation was further complicated by congenital absence of her maxillary left permanent lateral incisor, presence of a peg-shaped maxillary right lateral incisor crown and retained maxillary second deciduous molars. She also had a buccal crossbite on the right-hand side (Figure 1).
The panoramic x-ray confirmed the presence of the remaining permanent dentition, a dens-in-dente in the peg-shaped maxillary right permanent lateral incisor and insufficient space for restorative intervention to fully restore the congenitally absent maxillary left permanent lateral incisor.
Treatment plan and rationale
Arrangements were made for the collection of full records prior to assessment by the multidisciplinary team. Following the consultation, the recommended treatment plan comprised:
Provision of an upper removable appliance to restore aesthetics immediately and allow commencement of orthodontic treatment;
Endodontic re-treatment to replace the incomplete root fillings in the central incisors;
Extrusion of the maxillary central incisor roots to facilitate initial restoration with posts and composite crowns;
Open space to allow replacement of the congenitally absent maxillary left permanent lateral incisor with a dental implant.
The patient and parents consented to the treatment and undertook to achieve exemplary standards of oral hygiene.
Treatment progress
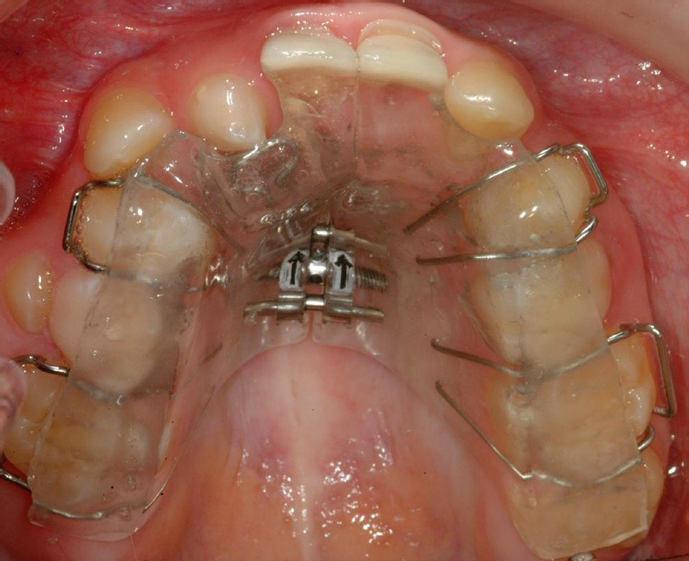
Initially, an upper removable appliance was placed for the first 7 months. This incorporated a biteplate to start to reduce the overbite and provide some space into which the upper roots could eventually be moved. A T-spring would start moving the instanding lateral incisor to a more favourable position, a midline expansion screw would start correction of the transverse problem and prosthetic acrylic teeth would temporarily restore dental aesthetics (Figure 2).
Figure 2. Modified upper removable appliance.
After crossbite correction and some overbite reduction was achieved, the central incisors were endodontically re-treated and stainless steel prefabricated posts were placed prior to coronal cores being built up with direct composite resin (Figure 3).
Figure 3. Serial periapical radiographs showing: (a) pre-treatment; (b) endodontic retreatment; and (c) post and core composite build-ups.
Subsequently, an upper and lower 0.022″ × 0.028″ pre-adjusted edgewise appliance was placed to level and align the arches initially with round, then subsequently rectangular, nickel-titanium archwire. After achieving levelling and alignment, the maxillary left canine was distalized with a nickel-titanium spring on a 19/25 stainless steel working archwire.
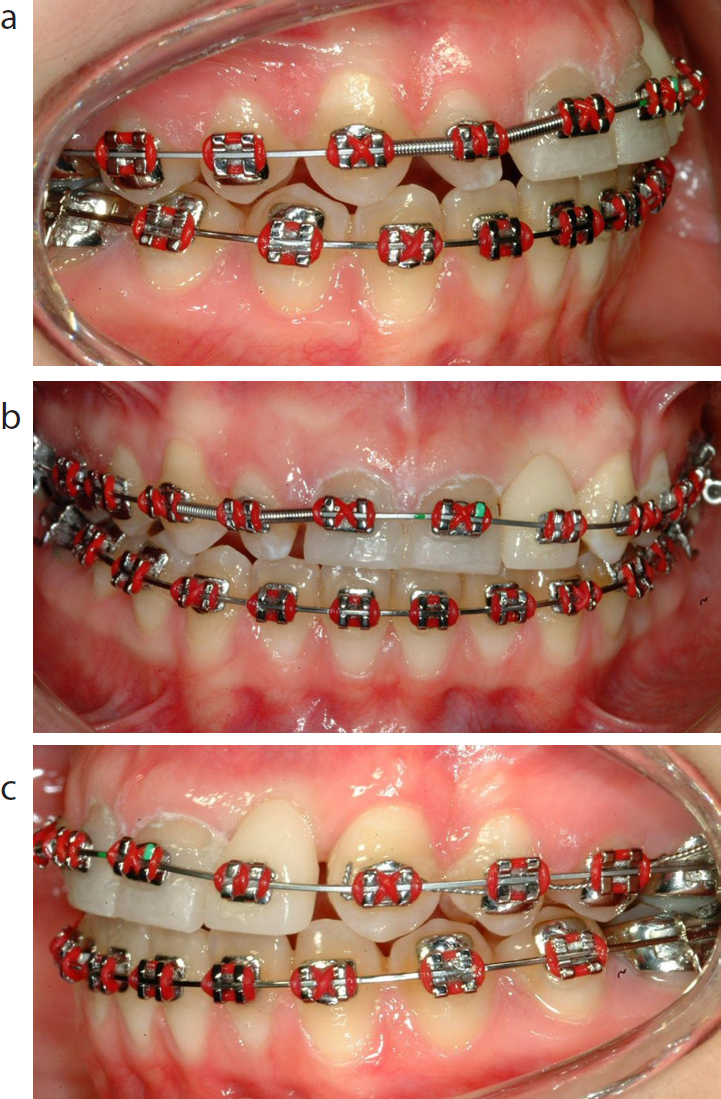
During the final stage of space opening, closed stainless steel coil springs were placed to maintain the recently opened spaces. An acrylic tooth was ligated to the stainless steel archwire to maintain aesthetics and maintain the opened spaces (Figure 4).
Figure 4.
(a–c) Orthodontic space opening in maxillary anterior region, and composite buildups after 24 months.
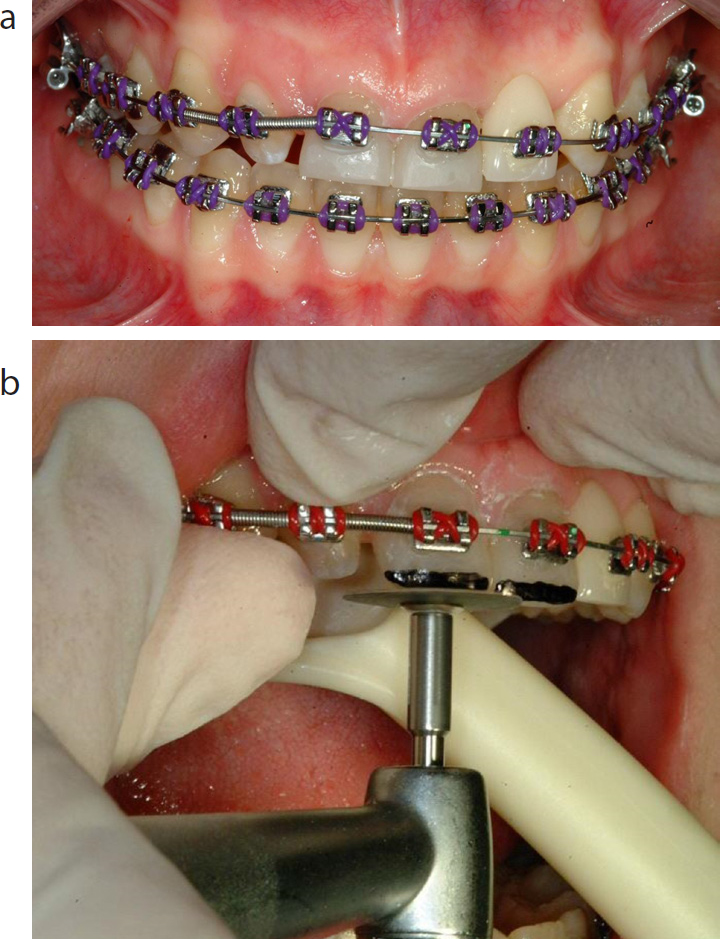
Gingival aesthetics in the maxillary anterior region was maximized by re-angulation of the brackets and selective grinding to allow extrusion of the incisors (Figure 5).
Figure 5.
(a) Extrusion of central incisors. (b) Selective grinding to allow further extrusion.
After 36 months of active orthodontic treatment, the fixed orthodontic appliances were removed. An upper modified Hawley and a lower Essix vacuum-formed retainer were fitted.
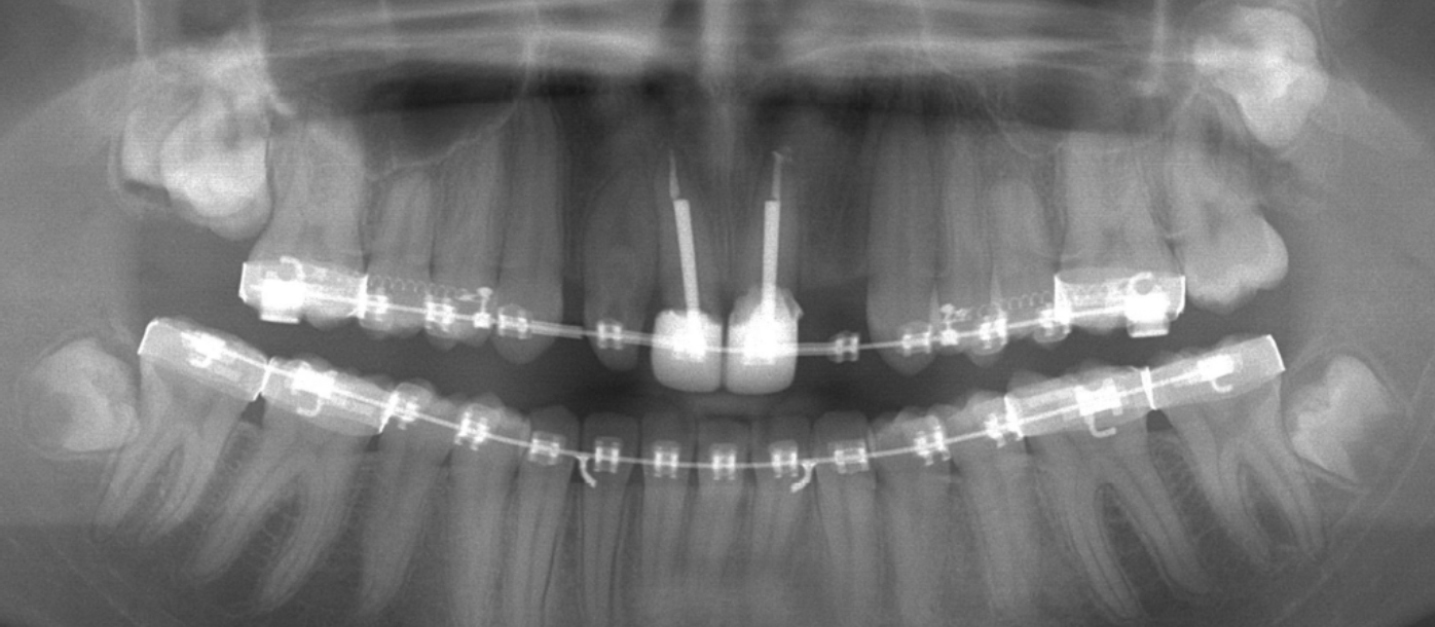
After a 6-month period of retention, the maxillary central incisors were definitively restored with laboratory made crowns. An implant-supported crown was placed in the maxillary left lateral incisor site, and the peg-shaped maxillary right lateral incisor was built up with direct composite resin (Figure 6).
Figure 6. Near end of treatment panoramic radiograph.
Discussion
Treatment was completed in 42 months (Figure 7). Initially, endodontic re-treatment was carried out, because of the poor quality of the root fillings provided immediately after the accident by the patient's GDP (Figure 3). It is generally accepted that the success rate of endodontic treatment will ensure good prognosis of the teeth, and it is positively correlated with the quality of the root filling.7,8,9 Furthermore, a number of reviews in the literature reported failures associated with post-retained restorations, 10% and 22%, over an average of 5-6 years follow-up.10,11
Figure 7.
(a–f) Post orthodontic/restorative treatment extra-oral and intra-oral views after 42 months.
The patient's perspective and many other clinical factors should be considered when deciding whether extraction or restoration of fractured teeth should be considered.12 Endodontic treatment and subsequent restoration may be vital with regard to preserving the alveolar bone for future implant placement, particularly important when teeth lie in a strategic position within the aesthetic zone.
After debonding this case, a satisfactory overbite, overjet and interdigitation was achieved. Root parallelism could be seen in the final panoramic x-ray, indicating a good prognosis for long-term stability.13 During the final stage of finishing, root divergence was ensured at the implant site to facilitate safe implant placement (Figure 6).
Historically, there have been many different treatment modalities to address a missing maxillary lateral incisor tooth:
Canine camouflage;
Tooth auto-transplantation; and
Prosthetic restoration.
Orthodontic space closure has the advantage of maintaining biological compatibility and avoids long-term dependence on prosthetic replacement but, in this case, this was an unrealistic option due to the Class I occlusion. In Class II malocclusions with an increased overjet, it is certainly appropriate to consider canine camouflage, which may result simultaneously in reducing the overjet. The decision to perform orthodontic space closure should therefore be taken into account: the occlusion, the degree of crowding and/or spacing and the width and root length of the lateral incisors, as well as the shape and shade of the canine crowns.14 Although all the treatment modalities mentioned come with limitations, in this case the dental implant placement was the ideal option to replace the missing tooth and to restore aesthetics and function to the maximum.
Conclusions
The success of treatment has been due to the meticulous treatment planning process which depends upon excellent lines of communication between the orthodontists and restorative dentists. A multidisciplinary approach involving both orthodontists and restorative dentists to provide endodontics, removable appliances, roots extrusion with fixed appliances, post and core build-ups, recreation of space for osseointegrated implant, restoration of the occlusion and final definitive restorations, allowed full rehabilitation of this patient's occlusion over a three-year period.
Without close liaison with all members of the multidisciplinary team none of this would have been possible.