Grover PS, Lorton L. The incidence of unerupted permanent teeth and related clinical cases. Oral Surg Oral Med Oral Pathol. 1985; 59:420-425
Ireland AJ. Familial posterior open bite: a primary failure of eruption. Br J Orthod. 1991; 18:233-237
Proffit WR, Vig KW. Primary failure of eruption: a possible cause of posterior open-bite. Am J Orthod. 1981; 80:173-190
Bosker H, ten Kate LP, Nijenhuis LE. Familial reinclusion of permanent molars. Clin Genet. 1978; 13:314-320
Brady J. Familial primary failure of eruption of permanent teeth. Br J Orthod. 1990; 17:109-113
DiBiase AT, Leggat TG. Primary failure of eruption in the permanent dentition of siblings. Int J Paediatr Dent. 2000; 10:153-157
Frazier-Bowers SA, Koehler KE, Ackerman JL, Proffit WR. Primary failure of eruption: further characterization of a rare eruption disorder. Am J Orthod. 2007; 131:578.e1-11
Frazier-Bowers SA, Simmons D, Koehler K, Zhou J. Genetic analysis of familial non-syndromic primary failure of eruption. Orthod Craniofac Res. 2009; 12:74-81
Decker E, Stellzig-Eisenhauer A, Fiebig BS, Rau C, Kress W, Saar K PTHR1 loss-of-function mutations in familial, non-syndromic primary failure of tooth eruption. Am J Hum Genet. 2008; 83:781-786
Sharma G, Kneafsey L, Ashley P, Noar J. Failure of eruption of permanent molars: a diagnostic dilemma. Int J Paediatr Dent. 2016; 26:91-99
Susami T, Matsuzaki M, Ogihara Y, Sakiyama M, Takato T, Sugawara Y, Matsumoto S. Segmental alveolar distraction for the correction of unilateral open-bite caused by multiple ankylosed teeth: a case report. J Orthod. 2006; 33:153-159
Partial or complete failure of tooth eruption may be due to several causes, including primary failure of eruption (PFE), and an accurate diagnosis is essential for appropriate management. This article reviews PFE and the possible treatment options. Case reports of two patients diagnosed with PFE are presented and their management discussed.
CPD/Clinical Relevance: Primary failure of eruption can be difficult to diagnose and differentiate from other causes of failure of eruption. This paper highlights the clinical presentation of PFE through a review of the literature and by illustration with two clinical cases.
Article
Failure of eruption of first and second molars is rare, with the prevalence estimated at 0.01% for first permanent molars and 0.06% for second permanent molars.1,2 Eruption failure may result from a number of causes. These include mechanical interference with eruption or failure of the eruptive mechanism of the tooth so that the expected amount of eruption does not occur.3 Mechanical failure of eruption (MFE) is characterized by single tooth anklyosis, whereas primary failure of eruption (PFE) is a condition in which unimpeded, non-ankylosed teeth fail to erupt with an absence of systemic factors.3 Primary failure of eruption is diagnosed based on its clinical appearance, which is reported to include the seven features shown in Table 1.3 The last of these clinical features has been disputed. Advances in gene discovery and identification have been able to show a heritable basis of this dental phenotype,4,5,6,7,8 and recently mutations in parathyroid hormone 1 receptor (PTH1R) have been identified in several familial cases of PFE.9
1. Posterior teeth are involved more than anterior teeth
2. Involved teeth may erupt partially and cease in eruption
3. Deciduous as well as permanent molars are likely to be involved
4. Involvement may be unilateral or bilateral
5. Ankylosis may be a secondary feature of involved teeth
6. Application of orthodontic forces is likely to cause ankylosis
7. There is no close familial or systemic association
Primary failure of eruption has been characterized further by Frazier-Bowers and colleagues,7 who described three different types:
Type I: showed all affected teeth to have a similar level of reduced eruptive potential;
Type II: included subjects for whom teeth distal to their most mesially affected tooth had a greater level, but still inadequate levels, of eruption;
Type III: included subjects who had a mixture of both types of PFE occurring in different quadrants.
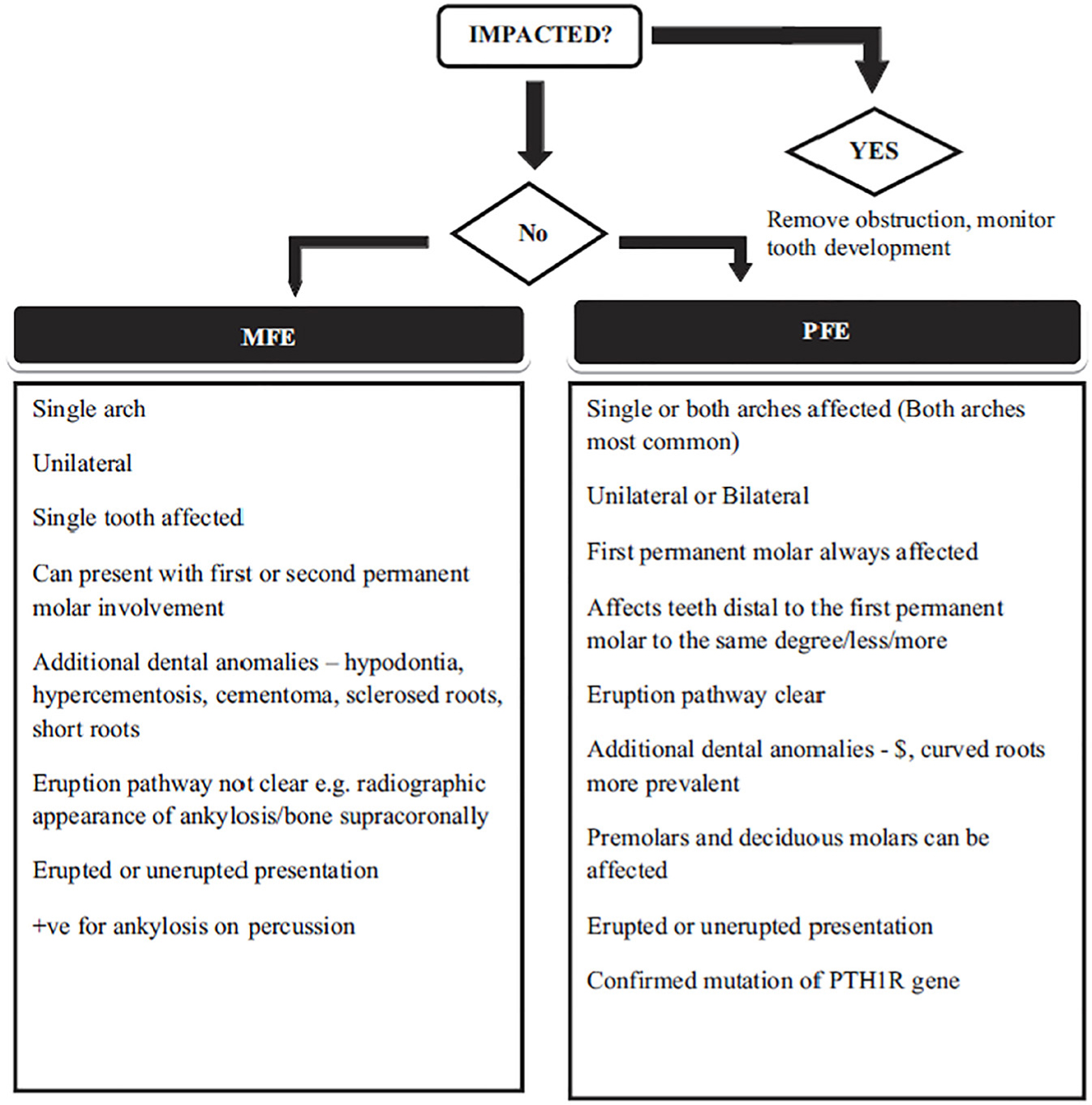
Previously, diagnosis between MFE and PFE has been difficult due to a lack of clear diagnostic criteria in the literature. A flow diagram was published by Sharma and colleagues to help clinicians with their decision-making regarding diagnosing PFE and MFE (Figure 1).10
Figure 1. A flow diagram to aid diagnosis of failure of eruption of the first permanent molar tooth/teeth.10
Treatment options
Treatment of patients with PFE can often be challenging. An interdisciplinary approach is required when considering the management of this rare condition. The various treatment options include:
Accept the infraocclusion;
Surgical repositioning of the affected area with a segmental osteotomy once growth has ceased, although limited success has been reported using this approach;11
Restorative correction of the occlusion once growth has ceased:
Coronal build-up or onlay of the affected teeth;
A removable prosthesis over the affected teeth.
Extraction of affected teeth and prosthetic replacement.
Exposing and bonding teeth affected by PFE is not advised as treatment via orthodontic forces has been suggested to lead to localized ankylosis.3
Case report
Patient 1
A 14-year-old boy was referred to the orthodontic department concerning his infraoccluded UR6 and LR6 with a resultant lateral open bite. The patient was concerned with the lack of eruption of the posterior teeth, although he did not have any aesthetic or functional concerns. The patient was medically fit and healthy and there was no family history of delayed eruption or failure of eruption.
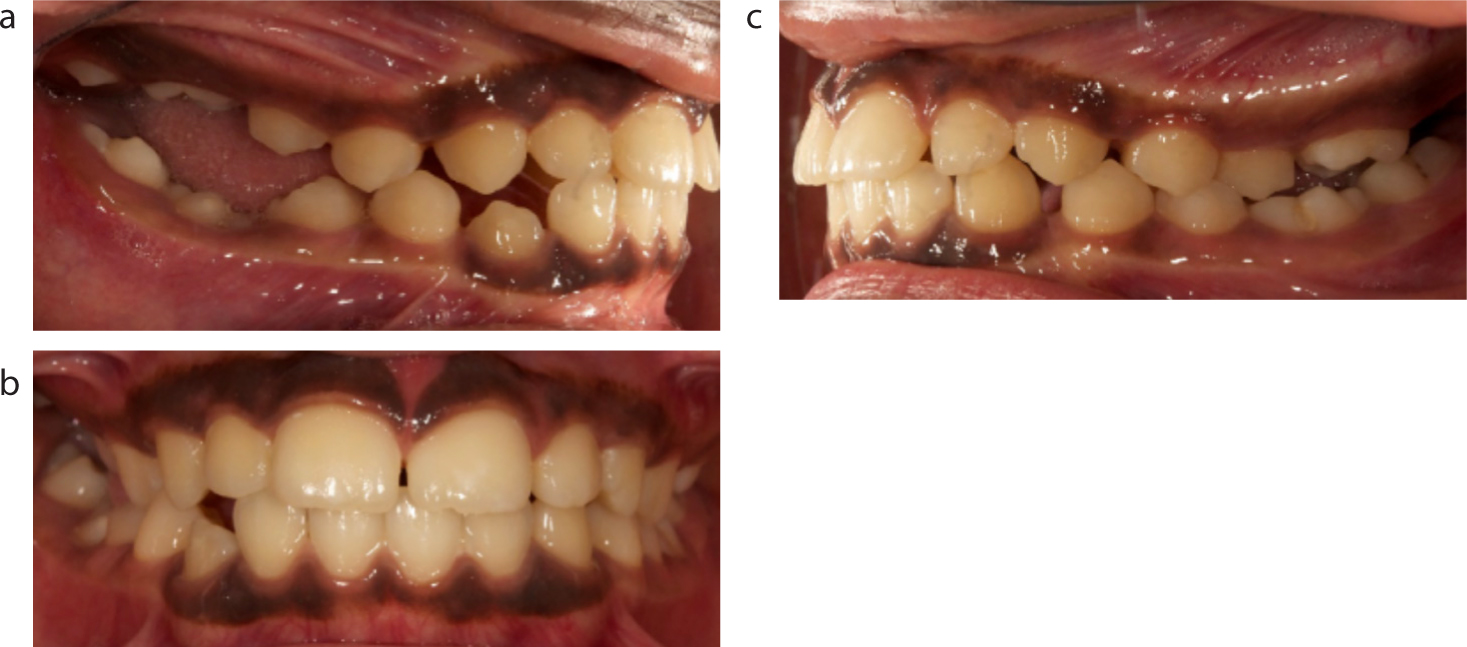
On examination, the patient presented with a Class I incisor relationship on a Class I skeletal base with average vertical facial proportions. Intra-orally, the patient was in the permanent dentition. The LR6, LR7, UR5, UR6 and UR7 were all infraoccluded with the uppers more severely affected than the lowers. There was a buccal crossbite present affecting the UL5 and LL6, with mesial occlusal contact present between the two. Whilst there was also a degree of infraocclusion affecting the UL6 and LL6, both teeth were in contact with the opposing dentition. Intra-oral photographs can be seen in Figure 2.
Figure 2.
(a–c) Intra-oral views of Patient 1 showing a mild lateral open bite on the left and a marked lateral open bite on the right.
A radiographic assessment was conducted which included a dental panoramic tomograph (DPT) and lateral cephalogram. The radiographs confirmed the clinical findings and show the severity of the infraoccluded teeth (Figure 3).
Figure 3.
(a) DPT and (b) lateral cephalogram radiographs of Patient 1.
The diagnosis of primary failure of eruption was made based on the non-eruption of both the UR56 and LR6 and all teeth distal to these. With mild infraocclusion affecting the UL6 and the non-eruption of the UL7, it was suspected that these teeth were also affected by PFE and, as such, both will be monitored to assess any further progression in their eruption. The position of the infraoccluded teeth was accepted and no active treatment was undertaken due to the limited chance of successful eruption under orthodontic traction. In addition, restorative treatment was not considered because the patient had no functional or aesthetic concerns.
The patient was made aware that, depending on his further vertical alveolar growth and the amount of infraocclusion, extraction of the most severely infraoccluded teeth might be required in the future due to difficulties in maintaining adequate oral hygiene. The infraocclusion is being monitored regularly by the patient's general dental practitioner using serial study models, repeated intra-oral photographs and measuring the level of the infraoccluded teeth relative to the adjacent teeth. Had the patient wanted restorative treatment to improve his aesthetics and function, composite build-ups or onlay restorations could have been considered as long as growth had been completed and following determination that the infraocclusion had stabilized. Due to the severity of the infraocclusion, it is unlikely that full correction of the lateral open bite could have been achieved.
Patient 2
A 17-year-old boy was referred to the orthodontic department concerning a partially erupted LR6. The patient's main concern was that he had a bad taste coming from this area, however, he had no aesthetic or functional concerns. The patient was medically fit and healthy and there was no family history of delayed eruption or failure of eruption.
On examination, the patient presented with a Class II division 2 incisor relationship on a mild Class II skeletal base with reduced vertical facial proportions. Intra-orally the patient was in the permanent dentition. The LR6 was severely infraoccluded and carious. The LR7 was partially erupted, mesially angulated and impacted on the distal aspect of the LR6 and severely carious. The LL7 and the UL6 were also infraoccluded. There was no contact distal to the second premolars on the right side and distal to the first premolars on the left side with resulting lateral open bites (Figure 4).
Figure 4.
(a–e) Intra-oral views of Patient 2 showing bilateral open bites.
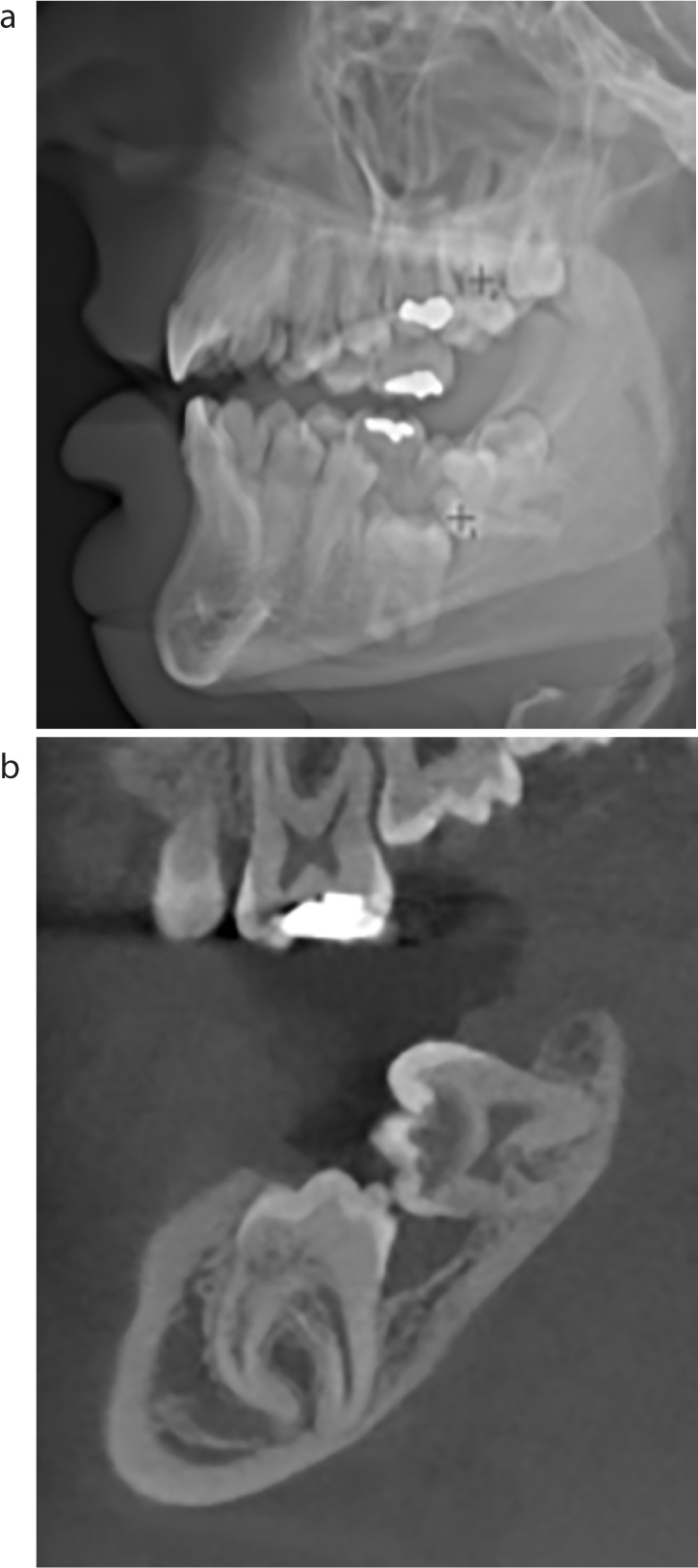
A Cone Beam CT (CBCT) of the right and left posterior regions was taken to confirm the extent of the infraocclusion and to identify the proximity of the lower molars to the inferior alveolar dental nerve (Figure 5). The CBCT confirmed the failure of eruption of the LR6 and shows it to be in close proximity to the lower border of the mandible.
Figure 5.
(a, b) A CBCT of Patient 2 showing the severely infraoccluded LR6 and mesially impacted LR7.
Following the CBCT, the patient was assessed on the joint orthodontic-paediatric clinic and diagnosed with PFE affecting the LR6, LR7, LL7, LL8, UL5, UL6, UL7 and UR7. Although the LL8 would not have been expected to be erupted at this point, it was felt that it would also be affected by PFE because all teeth distal to the most mesially affected tooth are affected. Different treatment options were considered, including accepting the infraocclusion, restorative management with either onlays or removable prosthesis or extraction of the affected teeth.
Whilst the vertical growth of both the maxilla and mandible for this patient is not yet complete, any further changes past the age of 17 are likely to be insignificant and certainly would not alter the posterior occlusion in a substantive way. One of the advantages of treating the lateral open bites with either composite onlays or partial dentures is that, should any further vertical growth occur, simple occlusal adjustments can be made to the composite or acrylic to restore a balanced occlusion.
The definitive treatment plan was based on the severity of the infraocclusion and patient preference and comprised the surgical extraction of the LR6, LR7, LL7, LL8 and occlusal onlays for the UL5 and LL6 to establish occlusal contact. In order to monitor the patient's vertical growth, which may give rise to further infraocclusion of the restored teeth, the patient will be reviewed by the restorative department. Should the patient present with an altered posterior occlusion, the composite restorations can be contoured or added to in order to maintain a well-balanced occlusion. Once the patient has reached the age of 18 and at the point of growth maturation, he may consider implants for restoration of the previously extracted teeth, with or without the extraction of the infraoccluded and restored teeth.
Conclusion
When faced with failure of eruption, it is important to be mindful of the true aetiology given the similar clinical presentations of PFE, MFE and impaction. Impacted teeth should erupt once the physical obstruction is removed, however, teeth affected by PFE and MFE will not. It is important to remember that applying orthodontic traction to teeth affected by PFE and MFE will not be successful and, indeed, may cause ankylosis.3 These two cases highlight the importance of accurate diagnosis and the implications for treatment planning.