Shaw WC, O'Brien KD, Richmond S, Brook P. Quality control in orthodontics: risk/benefit considerations. Br Dent J. 1991; 170:33-37
Tanki JZ, Naqash TA, Gupta A, Singh R, Jamwal A. Impacted maxillary incisors: causes, diagnosis and management. J Dent Med Sci. 2013; 5:41-45
Bharmal RV, Furness C, Slattery D, Campbell C. The multidisciplinary management of unerupted maxillary incisors. A report of three cases. Ortho Update. 2016; 9:122-128
Yaqoob O, O'Neil J, Patel S, Sheera J, Bryant C, Noar J, Gregg T, Morris D, Cobourne M. Management of unerupted maxillary incisors. Royal College of Surgeons of England. Faculty of Dental Surgeons. 2016;
Di Biase DD. Midline supernumeraries and eruption of maxillary central incisor. Dent Pract Dent Rec. 1969; 20:35-40
Bartolo A, Camilleri A, Camilleri S. Unerupted incisors – characteristic features and associated anomalies. Eur J Orthod. 2010; 32:297-301
Scott JH, Symons NBB. Introduction to Dental Anatomy, 9th edn. London: Churchill Livingstone, Medical Division of Longman Group UK Ltd; 1990
Pinho T, Neves M, Alves C. Impacted maxillary central incisor: surgical exposure and orthodontic treatment. Am J Orthod Dentofacial Orthop. 2011; 140:256-265
Crawford LB. Impacted maxillary central incisors in mixed dentition treatment. Am J Orthod Dentofacial Orthop. 1997; 112:1-7
Jauhar P, Machesney MR, Sharma K. Ingestion of an orthodontic archwire resulting in a perforated bowel: a case report. J Orthod. 2016; 43:237-240
Puyer J, McNamara C, Sandy J, Ireland T. An ingested orthodontic wire fragment: a case report. Dent J. 2016; 4
Unerupted maxillary incisors should be identified and managed promptly. When exposure and bonding of a gold chain to an unerupted tooth is indicated, there are multiple methods that can be used to apply traction to the tooth. This paper outlines the different methods available, their advantages and disadvantages and the important safety considerations. Treatment often utilizes small components which may pose an inhalation or ingestion risk if not used appropriately.
CPD/Clinical Relevance: This article reviews the different methods available to align impacted upper incisors. It details the advantages and disadvantages of each method and highlights the associated safety considerations.
Article
Unerupted maxillary incisors can have a large detrimental impact on dental and facial aesthetics which can subsequently affect patient psychology and self-esteem.1,2,3,4 Missing front teeth can also affect function and the developing dentition and therefore should be identified and managed as early as possible.3,4
The overall incidence of unerupted maxillary incisors has been found to be 2.6% in the referred population5 and is more common in males.6 The normal age of eruption of maxillary central and lateral incisors is 7−9 years.7 Eruption is considered to be delayed if:4
The contralateral teeth have erupted more than six months previously;
Both upper central incisors remain unerupted and the lower incisors have erupted more than one year previously;
There is a deviation from the normal eruption sequence.
The aetiology of delayed eruption can be hereditary or environmental, with common causes including supernumerary teeth, odontomes, previous trauma, early loss of deciduous teeth and retained deciduous teeth.4,8
The appropriate management of unerupted maxillary incisors is outlined by Royal College of Surgeons of England Guidelines4 and depends on the aetiology, patient age, stage of root formation and the amount of space available. Patients usually present in the mixed dentition, which poses anchorage and mechanical considerations when applying traction to these teeth.9
When exposure and bonding of a gold chain to unerupted maxillary incisors is indicated, there are multiple methods of applying traction to the tooth to facilitate eruption. These methods often utilize small components, such as a stainless steel hook attached to the gold chain, which can become loose and detach. This therefore poses important safety considerations due to the risk of inhalation/ingestion of the small hook component.
Clinical case
A male patient who was undergoing treatment for an unerupted maxillary central incisor attended the Orthodontic Department at the Eastman Dental Hospital reporting that the stainless steel hook attached to his gold chain had detached. He was asymptomatic but unsure what had happened to the hook. Following discussion and parental concerns, the patient attended his local hospital where an abdominal radiograph confirmed the presence of the hook in the stomach (Figure 1). The medical team advised monitoring the situation and the hook passed through his gut naturally with no complications. This case raises important considerations for the safety of applying traction to unerupted maxillary incisors via this method.
Figure 1. An abdominal radiograph showing the presence of a stainless steel hook in the patient's stomach.
In addition to this case, there have recently been published case reports of patients ingesting components of their orthodontic appliances which highlight the risks associated with such incidents and the surrounding safety considerations.10,11 In both of these recently published cases, the patients were undergoing fixed appliance treatment and fractured sections of their archwire were ingested. In one case, the patient experienced a perforated bowel which required surgery.10 In the other case, the archwire fragment passed through naturally with no complications, however, the patient still required a general anaesthetic initially to try and locate the archwire fragment.11 These cases highlight the potential severe risks associated with ingested components of orthodontic appliances and how every effort must be made to minimize these risks and their subsequent complications.
Although any components of an orthodontic appliance could come loose and be inhaled/ingested, it must be appreciated that this risk is increased when components are small and not an integral part of a fixed appliance, as can be the case with the appliances and mechanics used to treat unerupted maxillary incisors. Patients may inhale/ingest parts of their appliance unknowingly and can present with delayed symptoms. If any part of an appliance is missing or unaccounted for, a full history must be taken and appropriate patient/parental instructions given with regards to if or when to seek medical advice. The British Orthodontic Society has developed guidelines for the management of inhaled or ingested foreign bodies which should be followed alongside any local policies.12
Methods of applying traction
The methods of applying traction to unerupted maxillary incisors and the safety considerations for each method will now be considered. The advantages and disadvantages of each method are summarized in Table 1.
Advantages
Disadvantages
Sectional fixed appliance
No removable components
Rapid force decay of elastomeric traction when using powerchain or elastomeric thread, therefore need to see patient regularly
Less risk of small components being inhaled/ingested
Potentially reduced anchorage due to patient being in the mixed dentition
Less patient compliance required
May not be able to correct other occlusal discrepancies simultaneously
URA with archwire hook and intra-oral elastics
URA provides good anchorage
Increased patient compliance required
Can apply traction in different directions
Risk of an inhaled/ingested foreign body if ‘S’ hook comes loose
Continual force applied to unerupted tooth due to daily elastic change
Longer intervals between appointments due to continual force application
URA with elastomeric thread loop
URA provides good anchorage
Patient compliance required
No risks of inhalation/ingestion associated with using an ‘S’ hook
Force decay of elastomeric thread between appointments
Ability to apply traction in different directions
More regular appointments required
Applied force can be changed by altering length of elastomeric thread loop
The elastomeric thread can snap or unravel
URA with intra-oral elastics
URA provides good anchorage
Patient compliance required
No risks of inhalation/ingestion associated with using an ‘S’ hook
Force decay of the same elastic used between appointments
Ability to apply traction in different directions
More regular appointments required
No risk of elastic unravelling as with elastomeric thread loop
Only certain sizes of elastic can pass through the gold chain links − therefore less scope to control the length of elastic precisely and the subsequent level of force. Note: force control can be achieved by adjusting the length of the gold chain.
Magnets
Produces a measured continual force over a long period of time
Heat and hot liquids can cause the magnets to lose flux and thus lose force
Less frequent adjustment appointments are required than with mechanical eruption techniques
Corrosive properties of magnets
The position of the magnet can be changed to change the direction of the force
Sectional fixed appliance
This is often the method of choice due to its fixed nature and reduced need for patient compliance. As it does not rely on auxiliary hooks to apply traction, there is a reduced risk of components becoming loose and potentially being inhaled/ingested. However, it requires excellent oral hygiene and sufficient permanent teeth erupted to provide anchorage. A limitation is that it does not allow simultaneous correction of other occlusal discrepancies such as deep bites or crossbites. Removable appliances are an alternative in such patients.
An anterior sectional fixed appliance or a ‘two by four’ type appliance incorporating the upper first permanent molars can be used. Traction to the gold chain can be via elastomeric powerchain, elastomeric thread or an undersized, ‘piggyback’ nickel titanium archwire. Ideally, traction should only be applied once in a stainless steel archwire to prevent arch form distortion.
Upper removable appliance (URA) with archwire hook and intra-oral elastics
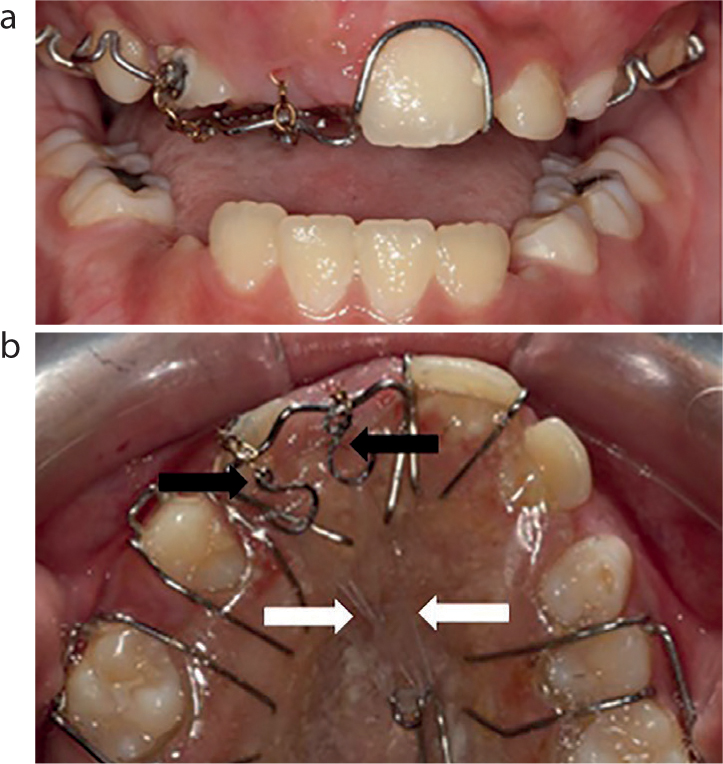
This is a common method of applying traction to an unerupted incisor, using a URA, a hook bent from an archwire section and intra-oral elastics to apply traction. Extra-orally an ‘S’ hook is bent from an archwire, commonly rectangular stainless steel (SS) or titanium molybdenum alloy (TMA). A 0.016” x 0.022” SS archwire is preferable due to being easy to form yet stiff enough to hold its shape. One end of the hook is attached to the end of the gold chain and ‘closed’ to attach it to the gold chain securely, the other end of the hook is left open. The patient attaches an intra-oral elastic from the open end of the hook to a hook on the URA (Figure 2). This elastic is changed daily to apply optimal traction to the unerupted tooth.
Figure 2.
(a, b) Two ‘S’ hooks (black arrows) used with intra-oral elastics (white arrows) and a URA to apply traction to UR1 and UR2.
Methods to increase safety
Form the hook from a rectangular archwire section to minimize the ends of the hook slipping over each other (more likely if a round wire is used);
Ensure that the closed end of the hook is fully secured via:
Crossing the closed ends of the hook over each other (Figures 3 and 4);
Turning the closed end of the hook back on itself (Figures 2 and 5)
Check the gold chain cannot pass through the closed end of the hook.
Figure 3. An ‘S’ hook fabricated by crossing the closed ends of the hook over each other (arrowed).Figure 4. An ‘S’ hook fabricated by crossing the closed ends of the hook over each other (black arrow) used with a URA and an intra-oral elastic (white arrow) to apply traction to the unerupted UR1.Figure 5. An ‘S’ hook fabricated by turning the closed end of the hook inwards (arrowed) to prevent the gold chain coming off.
Figure 3 shows an ‘S’ hook fabricated with the closed ends of the hook passed back and fully crossing over each other to ensure that the there is no space for the gold chain to come off the hook. This type of ‘S’ hook is shown in clinical use in Figure 4.
An alternative design of ‘S’ hook is shown in Figure 5 where the closed end of the hook is turned inwards so that it curls into a loop. This design of ‘S’ hook is shown in clinical use in Figure 2.
Alternatively, to eliminate the risks associated with using ‘S’ hooks, different methods of applying traction to the gold chain can be used.
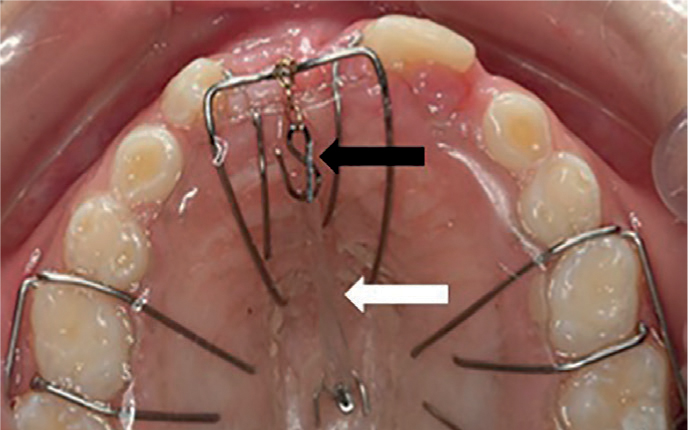
Upper removable appliance and elastomeric thread loop
This method uses a URA similar to the previous method. However, elastomeric thread is used to apply traction directly from the gold chain to the URA, without the use of a hook attached to the gold chain (Figure 6). The elastomeric thread is tied in a loop through the end of the gold chain and then looped around the palatal hook on the URA to apply traction to the tooth (Figure 7). The patient is not expected to change the elastomeric thread him/herself between appointments, therefore the same loop of thread is used to apply traction until the next appointment, when the clinician replaces the elastomeric thread.
Figure 6. A loop of elastomeric thread passed through the end of the gold chain. The loop of the elastomeric thread is then attached to a hook on the URA to apply traction to the unerupted tooth.Figure 7. A loop of elastomeric thread passed through the end of the gold chain and attached onto the hook on a URA (arrowed) to apply traction to the unerupted UR1.
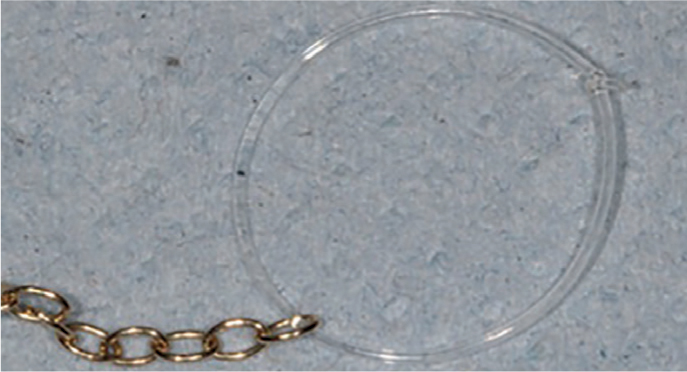
Upper removable appliance and intra-oral elastics
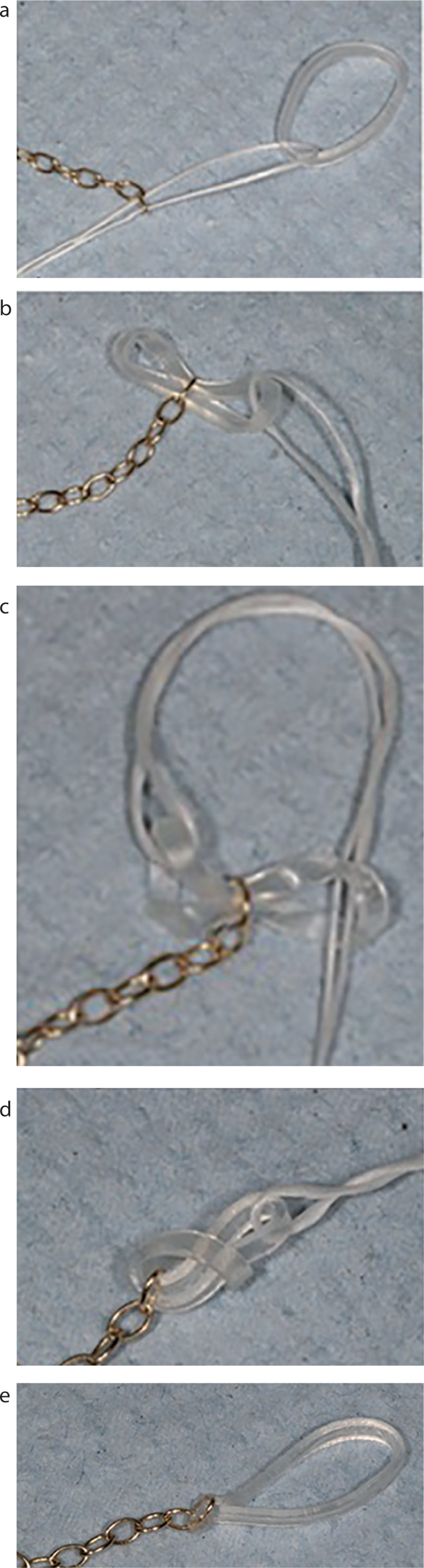
This method also eliminates the need to use an ‘S’ hook. This technique involves directly threading an intra-oral elastic through the end of the gold chain and passing the elastic back on itself to create a loop. This is attached to the palatal hook on the URA to apply traction to the unerupted tooth. Using dental floss as a guide allows the elastic to be passed through the gold chain link quickly and easily (Figure 8). Due to the ‘fiddly’ nature of placing the elastic, it is advised that the clinician places the elastic and the same elastic is used between appointments.
Figure 8.
(a–e) Dental floss can be used as a guide to thread an intra-oral elastic through the gold chain to create an elastic loop which can then be attached to a hook on a URA to apply traction to an unerupted tooth.
Magnets
An alternative to using mechanical traction is to use magnetic traction to facilitate the eruption of unerupted maxillary incisors.2 The magnets used are usually neodymium-iron-boron which produce static magnetic fields.2 This technique involves bonding a small magnet to the unerupted tooth and another magnet is incorporated into a URA worn by the patient.2 During the eruption process, the position of the magnet in the URA can be altered to direct tooth movement.
Finalizing alignment
To erupt and align an unerupted maxillary incisor may require using more than one of the techniques described above. Patients often require a URA initially to erupt the tooth, followed by a sectional fixed appliance to achieve a more acceptable alignment of the tooth until any further treatment is undertaken in the permanent dentition. It is important to appreciate that treatment for unerupted maxillary incisors is usually interceptive in nature due to the patient's age. Therefore the objective of the treatment is usually limited to erupting and aligning the unerupted tooth efficiently, and comprehensive correction of other features of the malocclusion can be addressed when the patient is more dentally developed.
Conclusions
Successful alignment of unerupted upper incisors is important for function, aesthetics, patient psychology and to prevent the development of further occlusal problems. Unerupted incisors should be identified and managed as early as possible to help achieve an ideal outcome. If exposure and bonding of the unerupted incisor is indicated, there are multiple methods of applying traction to the tooth. The advantages and disadvantages as well as the safety considerations of these options should be carefully considered when deciding which technique is most appropriate for each individual patient.