Patel A, Burden DJ, Sandler J. Medical disorders and orthodontics. J Orthod. 2009; 36:(Suppl)1-21
Radiation Protection 172: Guidelines on CBCT for Dental and Maxillofacial Radiology (Evidence-based guidelines). 2011;
Andreasen JO, Paulsen HU, Yu Z, Bayer T, Schwartz O. A long-term study of 370 autotransplanted premolars. Part II. Tooth survival and pulp healing subsequent to transplantation. Eur J Orthod. 1990; 12:14-24
Kindelan SA, Day PF, Kindelan JD, Spencer JR, Duggal MS. Dental trauma: an overview of its influence on the management of orthodontic treatment. Part 1. J Orthod. 2008; 35:68-78
Andersson L, Andreasen JO, Day P, Heithersay G, Trope M, Diangellis AJ International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 2. Avulsion of permanent teeth. Dent Traumatol. 2012; 28:88-96
Igarashi K, Mitani H, Adachi H, Shinoda H. Anchorage and retentive effects of a bisphosphonate (AHBuBP) on tooth movements in rats. Am J Orthod Dentofacial Orthop. 1994; 106:279-289
Spurrier SW, Hall SH, Joondeph DR, Shapiro PA, Riedel RA. A comparison of apical root resorption during orthodontic treatment in endodontically treated and vital teeth. Am J Orthod Dentofacial Orthop. 1990; 97:130-134
Levander E, Malmgren O. Evaluation of the risk of root resorption during orthodontic treatment: a study of upper incisors. Eur J Orthod. 1988; 10:30-38
Autotransplantation relies on successful interdisciplinary teamwork, utilizing the skills of each team member to optimize the outcome. During treatment planning, orthodontic input is required to determine whether orthodontic treatment is indicated and if a suitable donor tooth will be available. The orthodontist has a role in providing pre-surgical orthodontics to prepare the recipient site for the donor tooth and post-surgical orthodontics to correct the malocclusion fully and achieve the treatment goals. This article will outline the role of the interdisciplinary team members with an emphasis on the orthodontic aspects of treatment planning and the orthodontic treatment components of the autotransplantation pathway.
CPD/Clinical Relevance: Orthodontists have a key role in the autotransplantation team for both planning and provision of care. This article provides information for clinicians who wish to refer patients for autotransplantation or provide orthodontic care as part of the interdisciplinary team.
Article
One of the most challenging aspects of orthodontic treatment planning and delivery is the replacement of missing or poor prognosis teeth in growing children. Tooth transplantation has many advantages in the growing child, but success depends on careful case selection and treatment planning by a team with appropriate skills.
Interdisciplinary teamwork
To achieve an optimal outcome from autotransplantation, it is essential to involve clinicians from different specialties with specific skills. The potential roles of the various team members are outlined in Table 1, although this may vary between units. Both paediatric and restorative dentists may provide expertise in assessing poor prognosis teeth, recipient sites and donor teeth. Similarly, surgical procedures may be performed by paediatric dentists, restorative dentists or oral surgeons. The exact composition of the team should be developed to optimize skills to ensure an efficient care pathway with predictable outcomes. Within the team, the roles are defined to plan transfer of care at the appropriate time.
Specialty
Potential Role in Team
Paediatric Dentistry
Assessment of the prognosis of failing toothAssessment of recipient siteAssessment of donor toothProvision of surgical and restorative components of careMonitoring and follow-up of transplanted tooth
Orthodontics
Assessment of malocclusion and availability of donor toothOrthodontic treatment planningOrthodontic treatment
Restorative Dentistry
Assessment of the prognosis of failing toothAssessment of recipient siteAssessment of donor toothProvision of surgical and restorative components of care
Oral Surgery
Provision of surgical components of care
Radiology
Expertise in assessing the recipient site and donor tooth
Case selection
Autotransplantation teams are likely to receive referrals for assessment and treatment from a number of sources in primary or secondary care. The referral protocol should encourage referrers to consider a number of factors that may influence the patient's suitability for this treatment, mainly:
Patient factors:
Good dental health and ability to maintain this through long and complex treatment;
Willingness to attend multiple appointments and undergo extensive treatment;
Ability to accept surgical, restorative and orthodontic treatment;
Some understanding of the procedure, risks and long-term outcome, including potential failure.
Recipient site factors – alveolar bone volume and adjacent structures;
Presence of a malocclusion requiring extractions and willingness to undergo orthodontic treatment.
Following referral, the patient undergoes assessment by the autotransplantation team. This includes assessment of the patient's/family's wishes, including his/her motivation for treatment and a clinical assessment is carried out to determine suitability. Full orthodontic records are desirable to allow treatment planning prior to the interdisciplinary meeting.
Suitability for autotransplantation
Suitability for autotransplantation will be considered in terms of:
General considerations;
Need for tooth replacement;
Need for orthodontic treatment;
Availability of a donor tooth.
General considerations
As with any treatment, a thorough history is required to establish the concerns of the patient and family regarding whether treatment is likely to achieve the desired outcome. There are few medical problems that contra-indicate autotransplantation, although some conditions can make treatment difficult and complicated. For patients with bleeding disorders, poorly controlled diabetes, increased risk of bacterial endocarditis, a history of bisphosphonate use or malignancy, an opinion should be sought from their physician regarding suitability for treatment.1 Allergies to materials used in dentistry, such as nickel or acrylate, may be managed through the use of alternative materials. The dental history is important for determining suitability and likely compliance with care, specifically, attitude to dental treatment, caries risk, history of trauma, previous treatment and any evidence of anxiety towards treatment. Finally, any habits should be identified. Behaviours that increase the risk of trauma to anterior teeth, such as digit-sucking and nail-biting, need to be completely stopped prior to starting treatment to prevent unnecessary additional forces to the transplanted tooth.
Need for tooth replacement
Members of the interdisciplinary team jointly assess the need for tooth replacement. Opinion regarding the prognosis of a failing tooth may be provided by paediatric or restorative dentists based on clinical and radiographic signs and symptoms. Advice on the interpretation of radiographic signs may be sought from a dental radiologist. Predicting the long-term survival of traumatized teeth can be difficult, and any uncertainties about prognosis should be articulated to the patient and family during the decision-making process. Where teeth are missing, the existing method of tooth replacement is assessed for appearance, function and the patient's perception of its success (Figure 1). Tooth replacement with transplantation is only indicated where it is expected to provide a better outcome than the existing solution. In cases where no tooth replacement is required or an alternative method is deemed more appropriate, autotransplantation may be eliminated as a suitable option and the patient should be referred to the appropriate care pathway. Alternative treatment options are discussed fully later in the fourth article in the series.
Figure 1.
(a–d) A 14-year-old female who presented with a Class II division 1 malocclusion. A resin-bonded bridge (RBB) replaced the left maxillary left central incisor, which was absent following trauma. The patient was happy with the appearance of the RBB provided by her dentist and opted to keep this rather than undergo tooth transplantation. (e) Orthodontic treatment involved maxillary first premolar extractions and fixed appliances. The original bridge was still in situ after orthodontics and provided satisfactory aesthetics.
Suitability for orthodontic treatment
Suitability for orthodontic treatment is judged using the same criteria as for any other orthodontic patient, including dental health, oral hygiene, willingness to wear fixed appliances and ability to attend for appointments. It is essential that orthodontic treatment is judged to be beneficial and that the advantages of transplantation will outweigh the potential risk of increasing the length and complexity of orthodontic treatment. Orthodontic treatment need is assessed through routine extra-oral and intra-oral examination supported by special tests. An OPT provides an overall impression of the dentition and an indication of the stage of development of the donor tooth, bone height in the recipient site and the space available in the recipient site. A lateral cephalogram provides supplementary information to aid diagnosis and treatment planning. Additional 3D imaging, such as localized cone beam computed tomography (CBCT) techniques is often indicated to assess the donor tooth and recipient site in more detail. CBCT must be justified to aid diagnosis and inform the treatment plan2 (Figure 2). The clinical assessment allows diagnosis of all aspects of the malocclusion and formulation of a list of treatment aims. If the patient has no orthodontic treatment need or is deemed to be unsuitable for orthodontic treatment, it is unlikely that autotransplantation is a suitable treatment option and other types of care should be considered. For those requiring orthodontic treatment, the next stage of treatment planning involves identification of a suitable donor tooth.
Figure 2. Additional imaging aided assessment and planning for autotransplantation of a premolar from a crowded lower arch to manage maxillary arch hypodontia. (a, b) Pre-treatment: Class III incisor relationship with a reverse overjet in intercuspal position. The malocclusion is complicated by hypodontia affecting the maxillary lateral incisors and second premolars. The maxillary right primary second molar (URE) is restored with a stainless steel crown and has a poor long-term prognosis. The mandibular arch is crowded and the premolars are immature. (c) The preliminary plan was to accept the canines in the lateral incisor position and transplant the LR5 into the UR5 region. A CBCT was taken to assess the donor site bone height and proximity to maxillary sinus, alongside assessment of the root length and shape of the donor tooth (LR5). Due to the lack of available bone in the donor site, the plan was altered to distalize the UR4 with orthodontic treatment and transplant the LR5 into the UR4 space. (d) The transplanted tooth (LR5) in the UR4 position.
Availability of a donor tooth
Selection of the ideal donor tooth depends on the size of the recipient site and the desired coronal morphology of the tooth replacement (Table 2). The malocclusion may determine which teeth are extracted. Severely ectopic canine or premolar teeth that have been judged to be orthodontically unalignable may be considered as donor teeth but atraumatic removal can be challenging. In Class I malocclusions with crowding, or where space is required to recreate space for tooth replacement, extractions are often indicated. In these cases, consideration should be given to whether the extraction choice could provide a donor tooth. For Class I malocclusions without crowding and with adequate space for tooth replacement, it is unlikely that a donor tooth will be available (Figure 3). Class II malocclusions in growing patients may be treated by growth modification or orthodontic camouflage. In these cases, especially in the presence of crowding or significant incisor proclination, extractions are often indicated. Again, consideration should be given to extracting a tooth that could be used as a donor (Figure 4). Class III malocclusions requiring tooth replacement may be more challenging to plan, as it is often preferable to delay definitive treatment planning until future growth can be confidently predicted. In milder cases, amenable to camouflage, or cases with significant upper arch crowding, extractions may be planned. For those cases where treatment decisions must be delayed, it is important that space for tooth replacement is not lost.
Donor Tooth
Uses
Premolar
Replacement of central incisor, canine or premolar
Molar
Replacement of molar
Canine
Repositioning of grossly ectopic canineReplacement of central incisor, premolar or canine
Lower incisor
Maxillary lateral incisor
Figure 3.
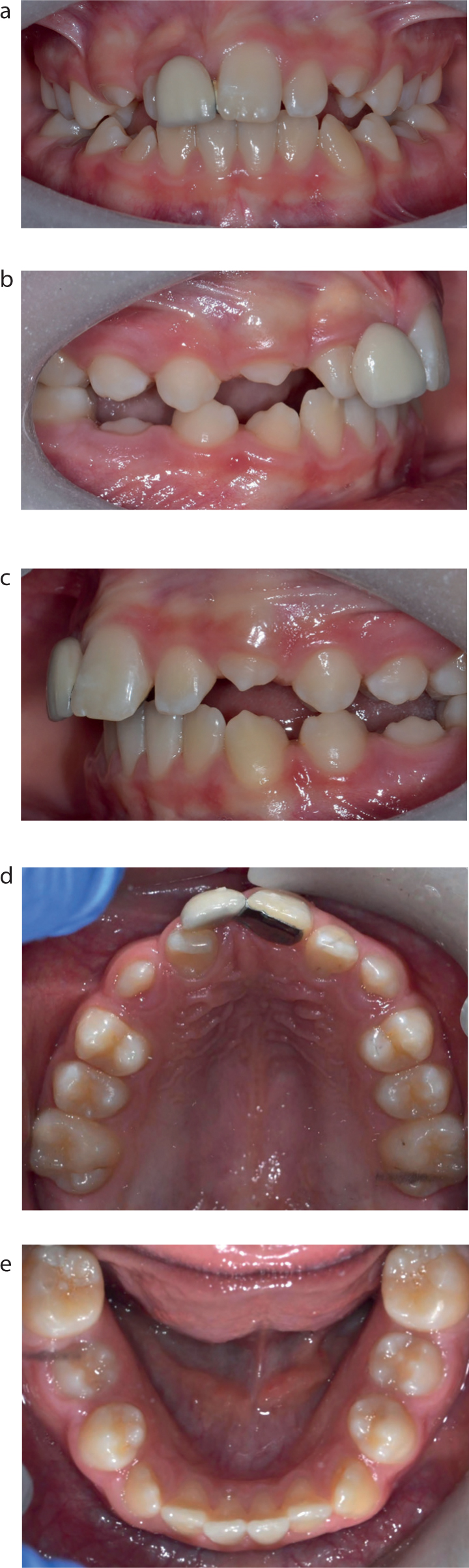
(a–e) A patient in the mixed dentition with an ankylosed UL1. The occlusion is largely Class I and this, combined with the lack of crowding, meant that the patient had need for orthodontic extractions and was therefore judged to be unsuitable for tooth transplantation.Figure 4. Tooth transplantation combined with functional appliance treatment. (Treatment provided by Claire Rooney). (a–e) Pre-treatment: 14-year-old male who presented with a Class II division I malocclusion and an 8 mm overjet. The maxillary right central incisor (UR1) was previously avulsed through dental trauma. A resin-bonded bridge was used to replace the missing UR1 but this failed to maintain the UR1 space.Figure 4.
(f–j) Functional phase of treatment to gain antero-posterior correction while aligning the upper anterior segment using a sectional fixed appliance.Figure 4.
(k–o) Following functional appliance treatment, assessment of the degree of crowding and incisor inclinations indicated extraction of all second premolars was required. The maxillary right second premolar was transplanted into the UR1 space and the patient underwent comprehensive fixed appliance treatment.
Orthodontic treatment for autotransplantation
Treatment planning is undertaken by the interdisciplinary team to ensure an efficient transition between components of care. The orthodontic treatment plan may involve both pre- and post-surgical stages. In some cases, the patient may require further dental development before being able to start treatment and the orthodontist may take responsibility for monitoring development.
Awaiting dental development
Autotransplantation has been shown to have the highest success when the donor tooth is transplanted when the root development is approximately 75% of expected length.3 However, if a very young patient loses a tooth due to dental trauma, an interim plan may be required. The aim of this treatment is to maintain space and to provide aesthetic and functional solutions, whilst awaiting dental development. The most common interim solution is a removable appliance with prosthetic teeth (Figure 5). Regular monitoring is essential to determine the ideal time for tooth transplantation and ensuring prompt care.
Figure 5.
(a, b) An interim denture used to maintain space following traumatic loss of the maxillary right central incisor in a young patient who required further dental development prior to autotransplantation.
Pre-surgical orthodontics
Pre-surgical orthodontics aims to create adequate space for the transplant and address aspects of the malocclusion that requires correction prior to the surgery. The antero-posterior, vertical and transverse elements of the malocclusion must be considered, as these influence space requirements, anchorage demands and treatment timing and sequencing. This may include correction of a significant antero-posterior or vertical discrepancy or centreline correction to ensure that the transplant can be placed in the correct position. Fixed, functional or removable appliances may be used, depending on the planned tooth movements. Staged extractions may help to create space for the transplant, correct crowding or address centreline discrepancies. Overbite reduction may be required to ensure that the transplant will not be placed in a position with occlusal contact post-operatively. Additional anchorage may be necessary to maintain space in staged extractions, or in cases where the donor tooth choice complicates the orthodontic treatment (Figure 6).
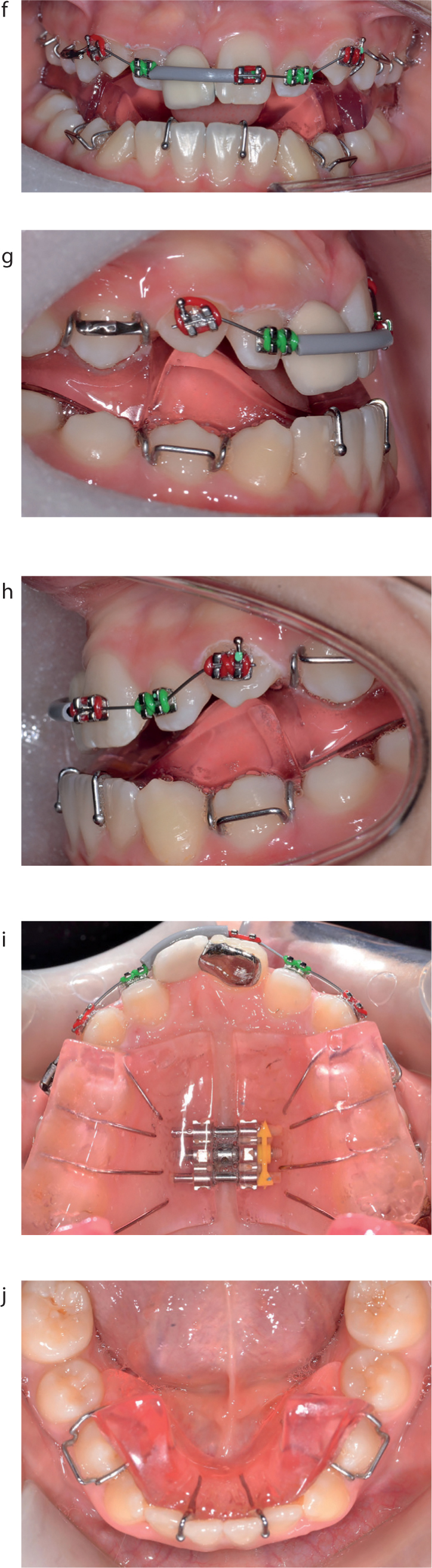
Figure 6. Anchorage support during orthodontics. (a) An OPT showing the malocclusion pre-operatively. The maxillary right central incisor had been lost following dental trauma with subsequent space loss. (b) A transpalatal arch with nance was used while creating space in the maxillary right central incisor position following extraction of the maxillary left first premolar.
Post-surgical orthodontic treatment
Following transplantation, it is recommended to wait a minimum period of 3–9 months prior to application of orthodontic force to the transplanted tooth. This is based on the guidelines for orthodontic treatment of avulsed teeth,4,5 although the underlying evidence in this area is relatively weak. Anecdotal evidence from teams in Europe suggests that earlier application of forces, after 8 weeks, can reduce the incidence of ankyloses, but this has not yet been demonstrated by research. The rationale for the length of delay in force application is a balance between promoting healing of the pulp and periodontal ligament and enabling force application before complete alveolar bone repair. In addition, in immature teeth, it is expected that some continued root development would be seen in this period to confirm satisfactory healing. The type of movement required on the transplant may also influence the timing of force application, with extrusion movements being commenced earlier than rotation or bodily tooth movement.6 In the healing period, orthodontic treatment may be continued for the remaining dentition to address other aspects of the malocclusion efficiently (Figure 7).
Figure 7. Orthodontic treatment is commenced in the mandibular arch while the transplant in the maxillary left central incisor position heals.
All transplanted teeth should undergo regular clinical and radiographic examination throughout treatment to assess pulp health, root development and root resorption. This follows an agreed protocol to avoid duplication but to ensure adequate monitoring. There should be a high index of suspicion for ankylosis and any abnormal tooth movement should be investigated promptly. Donor teeth with closed apices at time of transplantation will require pulp extirpation and a definitive root canal treatment post-operatively. There appears to be no increased risk of orthodontically-induced root resorption in root-treated teeth and some studies have even shown reduced levels of orthodontically-induced root resorption with root canal treatment.7 It is expected that root-filled transplanted teeth would behave similarly. Teeth transplanted with an immature root and open apex are expected to continue root development, but a normal root length may not be reached and the effect of orthodontically-induced root resorption may therefore be more significant.8 Prior to completion of orthodontic treatment, it is advisable to remove the interim composite camouflage and reassess the position of the transplanted tooth with a restorative dentist, to confirm the precise restorative camouflage required and how orthodontic finishing may assist this (Figure 8). Alterations in tooth positioning can provide space for the restoration and improve the gingival contour. Placing a first-order bend in the orthodontic wire can inset the transplant so that minimal labial tooth preparation is required, thus improving the bond strength of the final veneer restoration. Retention is a key component of the orthodontic treatment and should be planned with consideration of the initial malocclusion, tooth movements and any future restorative treatment that is planned. Removable retainers may require replacement as the transplanted tooth is reshaped. Bonded retainers may be complicated by the morphology of the transplanted tooth and adhesion to any coronal restorations that have been placed.
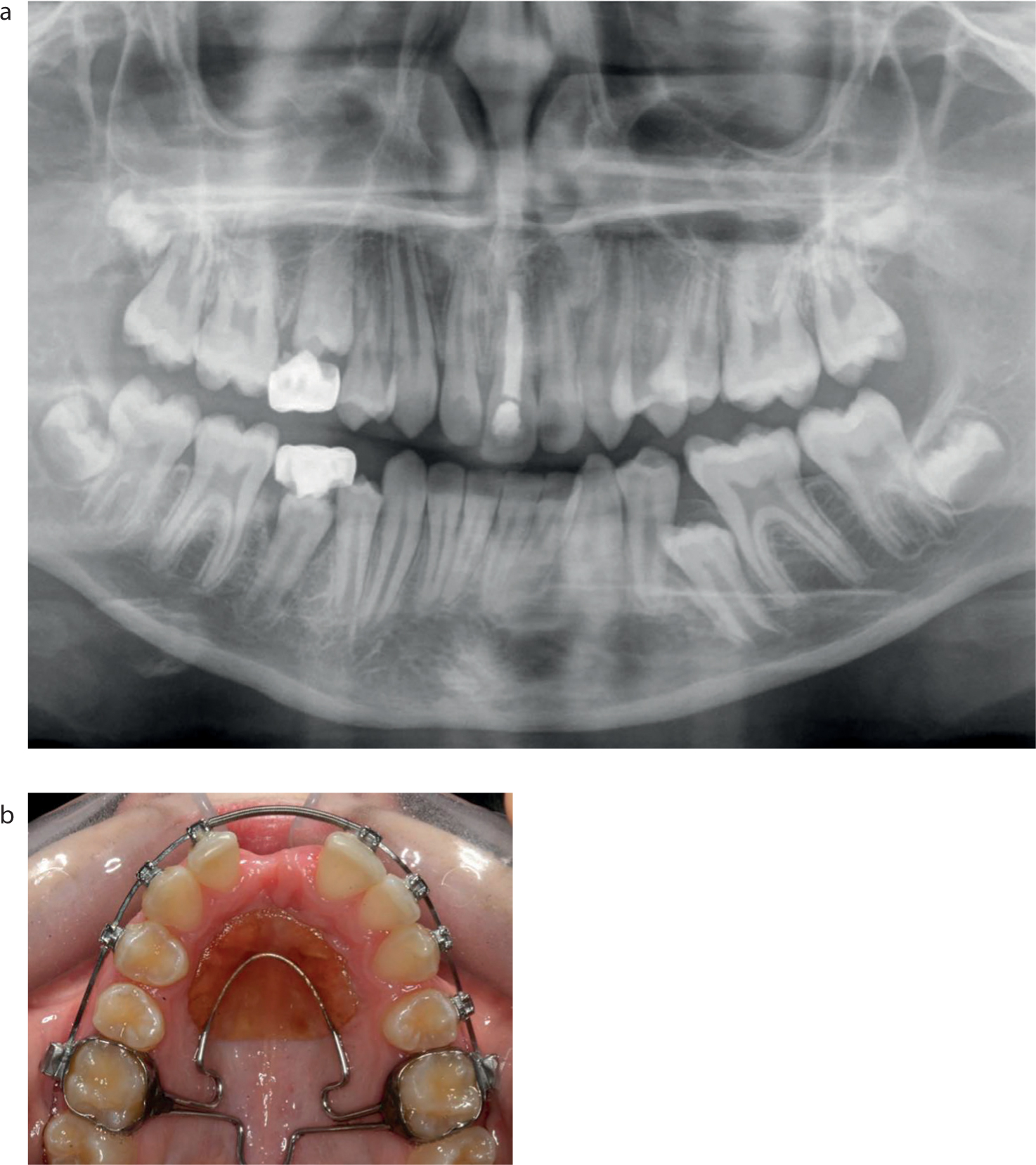
Figure 8. Removal of the interim composite camouflage aids final orthodontic positioning of the transplanted tooth. (a, b) A transplanted premolar in the maxillary right central incisor position with the interim composite restoration. (c, d) The transplanted tooth with the composite restoration removed to enable visualization of the crown and root to aid tooth positioning.
Conclusions
Orthodontics is an important component of autotransplantation treatment. A comprehensive orthodontic assessment is essential to determine treatment need and suitability based on the overall malocclusion, the availability of a suitable donor tooth and the feasibility of creating adequate space for transplantation into the recipient site. Orthodontic treatment has a role prior to transplantation, to prepare the recipient site, and after transplantation to fully correct the malocclusion.