Integrating lingual orthodontics into specialist practice Dental Update 2024 12:3, 707-709.
Abstract
Lingual orthodontics as a treatment modality has gained popularity over recent years as adults increasingly seek treatment to align their teeth, but with the minimum aesthetic impact in the process. This article will show how lingual orthodontics can be introduced into the clinical practice.
CPD/Clinical Relevance: Starting out with lingual orthodontics can be a daunting prospect and it comes with costs, including training, materials and inventory. It is important that clinicians should be aware of some of the factors to consider in ensuring these appliances are successfully integrated into clinical practice.
Article
Lingual orthodontics is an evolving treatment modality and increasingly an appliance of choice for the patient wanting discrete yet comprehensive treatment. Although historically not always a treatment of choice, lingual appliances have enjoyed an increase in popularity in recent years with the advent of contemporary lingual appliances providing a viable treatment alternative to aligner treatments and aesthetic labial brackets.1 It is estimated that about 10% of the UK's 960 registered orthodontic specialists offer the lingual technique, and the number is growing.2
Why undertake lingual orthodontic treatments?
In 2016, the British Orthodontic Society (BOS) conducted a survey designed to gather data about adult orthodontics in the UK, which was sent to all members working in specialist practice. Seventy-five percent of respondents reported seeing an increase in adult treatment, with a quarter starting more than 50 new adult cases each year, the main drivers for treatment appearing to be heightened awareness of adult orthodontics, alongside rising expectations on how treatment can positively impact on both appearance and well-being.3 This increase in demand for treatment, and in particular aesthetic treatment, has made the use of lingual appliances all the more appealing to the public and prompted more orthodontists to consider integrating the technique into clinical practice.
What are the advantages of choosing lingual appliances?
For the patient, the advantages of choosing lingual appliances mostly centre on the fact that all the attachments are provided lingually and so are hidden from family and friends (except on the odd occasion where the throwback of the head when laughing, or being shorter in stature could potentially reveal a glimpse of the appliances). As they are fixed, some patients do express a preference for these over removable aligner-type treatments, which require more compliance with wear.
For orthodontists, they are effective at managing a full range of malocclusions, including extraction cases, where aligners, despite their considerable advances in recent years,4 may not still be able to deliver fully.
How to integrate orthodontics into the clinical practice?
Undertaking and successfully integrating lingual orthodontic treatment into the clinical practice takes patience, perseverance and practise. It requires the purchase of new materials and instruments, appropriate training (including that of the team members) and time to learn and deliver the treatment. This article aims to give pointers to assist readers in successfully introducing lingual orthodontics into their armamentarium.
1. Appliance choice
The first thing to consider is what type of lingual appliance treatments the practice plans to introduce. A ‘2D’ type of appliance can be a good place to start, owing to the ease with which these can be used, the reduced cost (owing to lack of a laboratory fee as brackets are placed directly), and the limited amount of additional equipment inventory required.
2D appliances work well where treatment objectives are limited to tooth tipping and alignment. They can be a good option for incisor alignment or reduction of black triangles by incremental interproximal stripping in what would otherwise be aligner-type treatments. Simple crowding, including post-orthodontic treatment relapse, and simple alignment of the lower arch in deep bite cases where a labial appliance has been fitted in the upper but placing lower brackets might be troublesome, can also be good indications for 2D appliance use (Figure 1). Examples of these types of simple lingual appliances include 2D® (Forestadent, Pforzhiem, Germany) and the self-ligating bracket, Innovation–L (GAC, Birmingham, USA).
Figure 1.
(a–d) Patient attended with fractured bonded retainer on maxillary 4 incisors. Six months later with a sectional 2D® lingual appliance was ready for debond.
For greater control in cases requiring first-, second- and third-order movements, consideration needs to be given to an appliance that has prescription built into the brackets. Owing to the varied morphology of the lingual aspect of teeth, and the need for the teeth to be perfectly aligned on the opposite side to where the brackets are placed, requires the appliance to be customized and then be placed indirectly (Figure 2). Current popular examples of such appliances include Incognito™ (3M-Unitek, Top-Service für Lingualtechnik, Bad Essen, Germany), WIN (DW LingualSystems, Bad Essen, Germany) and the self-ligating system Harmony (American Orthodontics, Sheboygan, USA).
Figure 2.
(a–d) Patient attended with large maxillary diastema requiring bodily movement to close. Here Incognito™ is being used to close this down.
2. Patient selection and education
The cost of lingual appliances, especially those requiring laboratory fabrication, often self-selects patients as, for many, this treatment is financially out of reach.5 Beyond this, however, as a clinician wanting to integrate lingual treatments into the practice, the type of patient who would be suitable for this treatment modality needs to be considered. In the first instance, whilst learning, it is probably best to consider treatment complexity and opt for non-extraction cases. Certainly, this is advisable for 2D® treatments.6 As confidence is gained then increasingly more complex extraction cases can be managed and the full range of possibilities with customized appliances can be considered.
The second consideration is the patient personality. To start with, these treatments are going to take significantly longer to complete, both in overall treatment duration and the time of each individual appointment. The patient should be aware of this and patience is important.7
Thirdly, especially when starting out, patients who are relatively relaxed should be selected. It is probably wise to explain that, as a pioneer of this technique, both clinician and patient are ‘embarking on a new journey together’. It may be that this is reflected in the fee, to take the pressure off delivering the treatment, and enabling the clinician to make the most of all the learning outcomes encountered.
On a similar note, it may be best to learn this technique with those patients who are ambivalent to whether the appliance is labial or lingual. This allows the back-up of moving to labial mechanics if difficulties are encountered later (suggesting this later in treatment never inspires confidence and for many lingual patients this would not be an acceptable option as they only sought treatment in the first instance on the understanding that the appliance was to be discrete).
It is always important to meet patient expectations and, if it is felt from initial consultations that these can't be delivered, then do not embark on treatment and save later problems. Patients also need to be aware of the potential for tongue irritation and speech effects with lingual treatments (these are potentially less of an issue with the 2D® systems that are lower profile), and for those who could have an issue with this, possibly owing to the nature of their job, counselling should be offered accordingly.
Excellent record-keeping is essential and all relevant details of these discussions should be documented in the patient notes. In cases involving extractions, it is always worth delaying these, because of the risk of teeth moving into extraction sites and presenting problems with the indirect placement of the brackets. Also, this ensures that the patient can cope before irreversible changes are made to the starting malocclusion. Patient preparation is key for success in lingual orthodontics and, if managed well, patients will help build the practice further by word of mouth recommendation.
One note of caution though is that lingual patients have full visual access to scrutinize their treatments and will comment on every minute tooth movement that they perceive is not ideal. Be prepared for this and the fact that, once used to the appliances, they are seldom in a rush to have appliances removed. This is in contrast to patients having labial treatment, who eagerly await the day of debond. The lingual patients have weeks to get used to their smile and for them the clinician is likely to be just replacing one lingual wire with another smaller one, the bonded retainer.
3. Training
There is a steep learning curve when embarking on lingual orthodontic treatment and so it is a wise investment to consider what training courses are required to get started. An online search will reveal many possibilities. For some of the more popular appliances, certification courses exist,8,9 whilst other providers offer more generic courses.10,11
Hands on training provides important information about instruments required for effectively using the appliances, together with bonding protocols that have been well tested. Technique modifications include tooth surface preparation and discussing whether sandblasting is required, given the difficulty of removing some brackets at the end of treatment.
In addition, these courses suggest appropriate archwire sequencing, how to complete and send prescriptions, and they usually also cover the details of their follow-up client support, which is invaluable, especially in guidance through those first few cases.
After initial training, refresher courses from the major suppliers are usually available, along with advanced user groups. Meetings of the British Lingual Orthodontic Society (BLOS) are an ideal way to gain confidence and explore new ideas amongst peers. BLOS12 offers members discounts on training and materials, as well as member-only training events. Their website also offers the public a ‘find an orthodontist’ search function of its membership.
4. Inventory
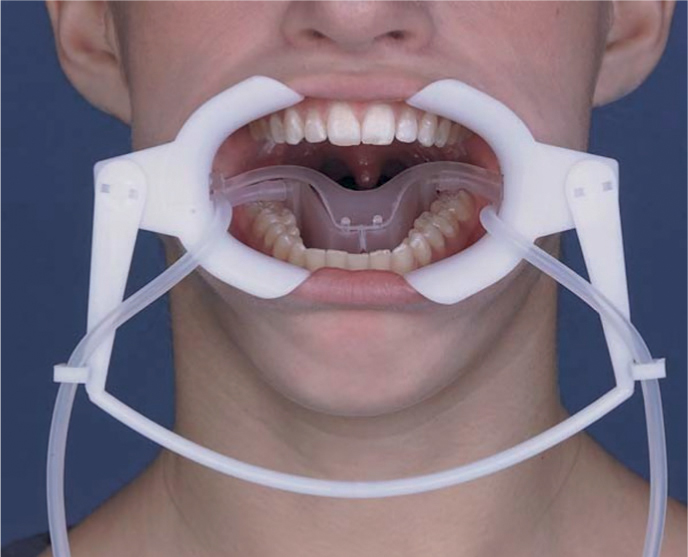
There will be a requirement for different instrumentation and materials when embarking on a lingual practice and the training courses will advise on these. This can range from a simple additional item, like the special explorer for the Forestadent 2D® system to open the bracket wings (Figure 3), to more extensive needs, such as the NOLA dry field system to isolate all the lingual surfaces adequately ahead of bonding customized appliances indirectly (Figure 4), and the use of a hydrophilic bonding agent such as Ortho Solo™, where moisture control is more difficult in lingual cases (Figure 5).
Figure 3. Special explorer with director to open 2D® brackets (Forestadent) for archwire insertion.Figure 4. NOLA Dry Field Retractor.Figure 5. Ortho Solo™ Universal Sealant and Bonding Enhancer
It is advisable to purchase specific lingual instruments which, although similar to their labial counterparts, are actually smaller and orientated to the lingual aspect for easier use. Lingual ligature directors can direct and torque archwires into the slot and lingual ‘cinch back’ pliers prevent archwires from slipping, or the ends from irritating the tongue (Figure 6).
Figure 6. Lingual NiTi distal ‘cinch back’ pliers.
Finally, many advocate the use of dental loupes to aid good posture and prevent the development of back and neck problems, as well as giving the ability to see the fine details of the lingual appliances which certainly aids their use.
5. Staff involvement
The move to lingual treatment puts everyone on a new learning trajectory and, for successful integration, ‘buy-in’ is needed from all staff members:
Receptionist, who will field callers with initial enquiries and make arrangements for those patients already in treatment who have queries, or those who require an urgent appointment.
Treatment co-ordinators who will be required to discuss lingual treatment options candidly prior to the patient being seen for consultation and answer questions.
Nurses and orthodontic therapists who, between them, may be taking impressions and scans, submitting all records for those appliances needing laboratory construction and fitting and adjusting appliances.
In order for this to work effectively, staff training and appointment scheduling are important. If not done ‘in house’, some companies offer this training as part of a suite of courses,13 whilst other companies tailor their training specifically to the team.14 Good staff training and delegation of roles helps everyone remain keen and motivated to promote the lingual treatments and get proficient at providing them.
6. Timing
The first cases undertaken will take much longer, so allow for this. Book the first lingual patients at the end of the session so that the pressure to get the next patient in is avoided. Treating patients with lingual appliances can be physically demanding and it is important to develop good posture from the start to avoid back problems. It may be advisable not to book consecutive lingual appointments until very familiar with the demands of this technique.
Ideally, adequate provision for lingual patients should be made in the diary for unscheduled visits. Emergency appointments for lingual patients can take considerably longer than expected. Additionally, lingual patients can be especially demanding about being seen promptly if they perceive treatment is not going in the right direction. This can be frustrating, especially in cases where there has been a considerable improvement to the initial presenting malocclusion and so patience and reassurance is required.
Finally, be available to answer questions that patients may have after they have left the surgery, and make effective arrangements to cover any emergencies that may arise between appointments.
7. Patient education
Patients may be unfamiliar with lingual treatment options. It is worth having a lingual typodont available so that the patient can see and feel with their fingers what the appliance is like. This is an opportunity for the merits of this treatment to be explained to the patient, especially if other appliance typodonts are available, along with the downsides, such as speech effects and temporary tongue irritation.
It is also an opportunity to explain about the complexity of providing treatment from the lingual aspect as well as the technology that goes into constructing the appliances (in particular those that are customized)15 and this can help prepare the patient for the discussion of the fee.
8. Pricing
The cost of lingual treatments will vary depending on case complexity and fabrication cost, with customized appliances obviously being more expensive. Pricing is a personal consideration but the BLOS website16 suggests that, for single arch treatments (for example requiring limited movements, eg post relapse treatment, or sectional appliances involving just the anterior teeth), fees may start around £2,000−£3,000 and customized appliances for definitive treatments typically start from approximately £6,000 up to around £10,000. Given the increased costs, compared to labial appliances, it may be advantageous to consider offering finance arrangements to help patients spread out the cost of treatment, if this is not already available. It is also important to make sure that any fees for laboratory construction of customized appliances are paid for ahead of their construction.
9. Marketing
Integrating a new treatment modality into the clinical practice needs to be planned very carefully. For those early lingual treatments, it will be important to follow-up case progress closely, evaluating results and the learning outcomes obtained along the way.
Patient feedback questionnaires may be of value in assessing patient experience of treatment and this can be correlated with patient expectations. As with all patients, good clinical records should be taken and then, as proficiency and confidence is gained, it will be possible to consider marketing to increase the size of the lingual practice. With appropriate consent, the clinical records and testimonies of ‘satisfied patients’ will be invaluable, as well as individual patient personal recommendations.17
Conclusion
Lingual orthodontic treatment, if managed and integrated well into the clinical practice, is an opportunity to increase options for patients to receive discrete treatment for a full range of malocclusions.
It will also add to the professional satisfaction of both the practice and the team as everyone learns to deliver quality treatments with whichever lingual system is being introduced.