Cedro M, Moles DR, Hodges S. Adult orthodontics in the absence of orthognathic treatment: a hospital perspective. J Orthod. 2012; 39:292-302
Claman L, Alfaro MA, Mercado AM. An interdisciplinary approach for improved esthetic results in the anterior maxilla. J Prosthet Dent. 2003; 89:1-5
Ong MM, Wang HL. Periodontic and orthodontic treatment in adults. Am J Orthod Dentofacial Orthop. 2002; 122:420-428
Kalia S, Melsen B. Interdisciplinary approaches to adult orthodontic care. J Orthod. 2001; 28:191-196
Melsen B, Agerbaek N, Markenstam G. Intrusion of incisors in adult patients with marginal bone loss. Am J Orthod Dentofacial Orthop. 1989; 96:232-241
Chasens A. Periodontal disease, pathologic tooth migration and adult orthodontics. N Y J Dent. 1979; 49:40-43
Johal A, Ide M. Orthodontics in the adult patient, with special reference to the periodontally compromised patient. Dent Update. 1999; 26:101-108
Dersot JM. Gingival recession and adult orthodontics: a clinical evidence-based treatment proposal. Int Orthod. 2012; 10:29-42
Sanders NL. Evidence-based care in orthodontics and periodontics: a review of the literature. J Am Dent Assoc. 1999; 130:521-527
Vardimon AD, Nemcovsky CE, Dre E. Orthodontic tooth enhances bone healing of surgical bony defects in rats. J Periodontol. 2001; 72:858-864
Zimmer B, Seifi-Shirvandeh N. Changes in gingival related to orthodontic treatment of traumatic deep bites in adults. J Orofac Orthop. 2007; 68:232-244
Re S, Cardaropoli D, Abundo R, Corrente G. Reduction of recession following orthodontic intrusion in periodontally promised patients. Orthod Craniofac Res. 2004; 7:35-39
Upadhyay M, Nagaraj K, Yadav S, Saxena R. Mini-implants for en masse intrusion of maxillary anterior teeth in a severe Class II division 2 malocclusion. J Orthod. 2008; 35:79-89
Carano A, Stefano V, Leone P, Siciliani G. Clinical application of the miniscrew anchorage system. J Clin Orthod. 2005; 1:1-8
Pinho T, Neves M, Alves C. Multidisciplinary management including periodontics, orthodontics, implants, and prosthetics for an adult. Am J Orthod Dentofacial Orthop. 2012; 142:235-245
Ericsson I, Thilander B. Orthodontic relapse in dentitions with reduced periodontal support: an experimental study in dogs. Eur J Orthod. 1980; 2:51-57
Zachrisson BU. The bonded lingual retainer and multiple spacing of anterior teeth. Swed Dent J. 1982; 15:(Suppl)247-255
Loss of periodontal attachment in adults usually manifests as pathological migration, traumatic deep bite and irregular dental spacing, which lead to compromised aesthetics and function.
This article describes the interdisciplinary management of an adult patient presenting with severe periodontitis accompanied by marginal bone loss and pathological migration of the upper right anterior teeth. The combination of a modified intrusion procedure of the upper anterior teeth and periodontal therapy led to significant improvement in function and aesthetics.
CPD/Clinical Relevance: The modified intrusion technique described in the present case can be a useful alternative to improve the periodontal condition as well as the aesthetics in periodontally compromised adult patients.
Article
Santosh Kumar
The number of adult patients seeking orthodontic treatment has increased significantly during recent years, which may be attributed to improved dental services and greater dental awareness among adult patients.1 The main motivating factors in adults seeking orthodontic treatment are a desire to improve their dento-facial aesthetics and function.2
The fact that the incidence of periodontal disease increases with age means that dental practitioners are more likely to see adult patients with periodontal problems. Periodontal disease usually manifests as tooth mobility, pathological migration, irregular dental spacing, and marginal gingival recession. Other features include drifting of teeth, missing teeth, proclination of the upper labial segment, rotations and over-eruption, which lead to functional and aesthetic problems. Where these features affect the maxillary anterior region, this will particularly result in compromised aesthetics.3
Orthodontic tooth movement in periodontally compromised patients differs considerably from that found in routine orthodontics. Loss of alveolar bone height leads to apical relocation of the centre of resistance. If the centre of resistance moves apically, the tipping moment produced by the force increases, therefore light force and relatively larger countervailing moment produced by a couple applied to the tooth would be necessary to effect bodily movement. A periodontally compromised dentition may also provide inadequate anchorage, provoking further bone loss. Micro-implants may be used as a useful source of anchorage in such cases. Judicious interdisciplinary treatment planning, regular periodontal care during active orthodontic tooth movement and establishing appropriate retention after orthodontic treatment are crucial for successful treatment outcome.4
Intrusion of incisors in adult patients with marginal bone loss offers a beneficial effect on the periodontium at the clinical and radiographic level.5 This article describes interdisciplinary management in an adult patient with severe periodontitis, where an intrusion procedure of the anterior teeth was modified to improve the periodontal condition surrounding the upper anterior teeth.
Case report
A 40-year-old male patient was referred by the Department of Periodontics. The patient's chief complaint was spacing and elongation of the upper front teeth. The patient had a history of severe periodontal disease, particularly affecting the upper right central and lateral incisors and upper right canine. This had been treated over a period of 6 months by subgingival scaling and root planing. After the active periodontal therapy, the affected teeth were splinted to promote healing and reduce the mobility. The patient was on regular periodontal maintenance therapy for 4 months.
Extra-oral clinical examination revealed a moderate skeletal Class II pattern, convex facial profile, acute nasolabial angle and lip incompetence. The vertical proportions of the face were within the normal limits. No remarkable facial asymmetry was seen. Intra-orally, the upper right central and lateral incisors and canine had undergone extrusion and occlusal trauma. There was localized gingival recession, no bleeding on probing and 3–4 mm pockets in relation to the splinted teeth. The splinted teeth were grade I mobile.
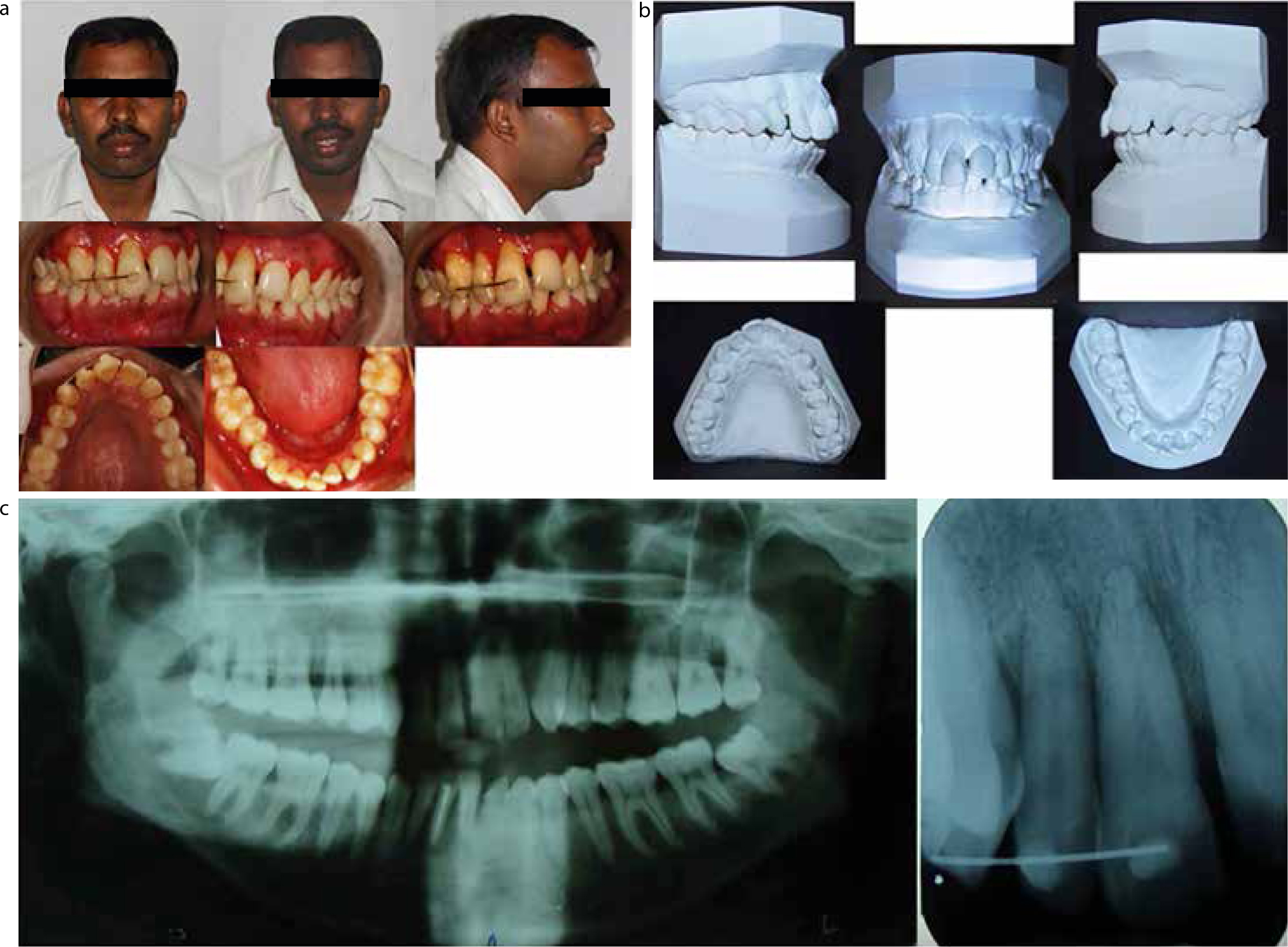
There was a Class I molar relationship bilaterally, deep bite, mild upper labial segment spacing and mild crowding in the lower arch. Both upper and lower incisors were labially inclined and incisors were in Class II division 1 relationship. The overjet and overbite were 5 mm and 7 mm, respectively (Figures 1a, b).
Figure 1.
(a–c) A 40-year-old male patient showing moderate skeletal Class II pattern, convex facial profile, bilateral Class I molar relationship, Class II division 1 incisors, deep bite, mild upper labial segment spacing and generalized bone loss extending to the apical third of the root length, particularly around the extruded maxillary anterior teeth.
Radiographic examination revealed generalized bone loss extending up to the apical third of the root lengths, particularly around the extruded maxillary anterior teeth (Figure 1c).
The treatment objectives
To correct the traumatic deep overbite;
To close the upper labial segment spacing and normalize overjet and overbite;
To restore aesthetics and function.
Treatment plan
Treatment options were discussed with the patient in detail. These were as follows:
Treatment alternative 1 (comprehensive treatment plan)
Intrusion of the upper right central and lateral incisors and upper right canine using fixed orthodontic appliance;
Levelling and alignment of both arches, followed by lingual retraction of the anterior teeth by extracting maxillary and mandibular first premolars were planned to correct the lip incompetency and normalize the facial profile;
Use of micro-implant to provide absolute anchorage for intrusion and maximum retraction;
Continuous monitoring of periodontal health with periodic scaling and root planing during orthodontic treatment;
Retention with a fixed lingual retainer;
Further periodontal treatment (eg free gingival graft placement) to enhance the root coverage in the upper labial segment.
Treatment alternative 2 (compromised treatment plan)
Stage 1
Intrusion of the upper right central and lateral incisors and upper right canine using a periodontal splint and micro-implant.
Stage 2
Upper fixed appliance to level and align, correct the incisor inclinations and close the upper labial segment spacing;
Maintenance of periodontal health during and after the orthodontic treatment;
Retention with a fixed lingual retainer;
Further periodontal treatment to enhance the root coverage in the upper labial segment.
The patient's primary concern was spacing and elongation of the upper right central, lateral incisors and canine. He expressed no concerns regarding the crowded mandibular teeth and requested upper arch treatment only. Therefore, treatment alternative 2 was chosen. No lateral cephalogram was taken as treatment was limited to the upper arch. Before commencement of treatment, there was close liaison between the Departments of Orthodontics and Periodontics to confirm that the periodontal disease was stable and it was appropriate to commence orthodontic treatment.
Treatment progress
Stage 1
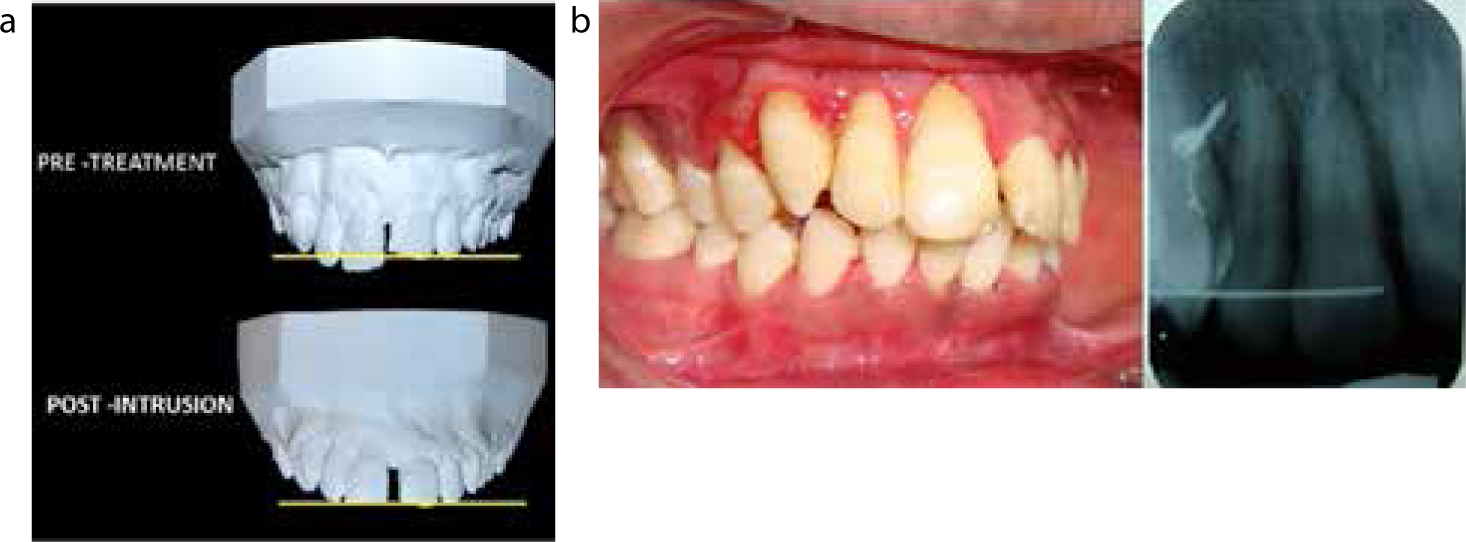
During the first stage of the treatment, the previously placed splint was replaced with a 0.019” × 0.025” stainless steel archwire which was bonded directly to the labial surfaces of the upper right central, lateral incisors and canine to act as a rigid periodontal splint. An intra-oral periapical film was taken using the long cone paralleling technique to assess the root positions of the upper right lateral incisor and canine, which showed adequate inter-radicular space near the apical third root lengths of both these teeth. A self-threaded micro-implant (length: 9 mm; diameter: 1.3 mm; SK Surgical, India) was placed in the alveolar bone between the apical third root lengths of the upper right lateral incisor and canine. The high placement of micro-implant also provided sufficient working distance for the elastics to intrude the incisors. An 0.010” ligature wire was ligated to the micro-implant to form a loop. Elastic thread was tied between the loop and the splint (between lateral incisor and canine) to apply a force of 15 grams to intrude the splinted teeth as recommended by Melsen et al (Figure 2).5 The elastic thread was replaced every 6 weeks to maintain adequate intrusive forces, as measured by a Dontrix Strain Gauge (Ortho-Care Ltd, Bradford, UK). A total of 3 mm of intrusion was achieved in 5 months, which was measured in the form of overbite reduction, using the incisor edges of the contra-lateral central and lateral incisors as a reference. Post-intrusion an intra-oral periapical radiograph, taken using the long cone paralleling technique, indicated maintenance of sufficient bone support with no signs of significant root resorption (Figure 3a, b).
Figure 2. A micro-implant was placed between the upper right lateral incisor and canine and elastic thread was tied to the rigid stainless splint to apply an intrusive force.Figure 3.
(a, b) Post-intrusion view and radiograph showing correction of the deep bite and maintenance of sufficient bone support with no signs of significant root resorption.
Stage 2
During the second stage of the treatment, the upper arch was bonded from first molar to first molar with a 0.022” × 0.028” pre-adjusted edgewise appliance (MBT) and levelling and alignment was initiated with a 0.012” NiTi wire. The archwire sequence during levelling and alignment was 0.012” NiTi wire, 0.014” NiTi wire, 0.016” NiTi wire, 0.018” NiTi wire and 0.018 × 0.025” stainless steel wire. Levelling and aligning was achieved in 3 months. Space closure commenced on a 0.019” × 0.025” stainless steel wire using elastic chain from canine to canine (Figure 4). The elastic chain was replaced every 6 weeks.
Figure 4. Upper anterior space closure with elastic chain.
During orthodontic treatment, the patient was motivated and periodontally maintained by the dental hygienist on a monthly basis. Space closure was completed in 4 months. Following completion of the orthodontic treatment, the upper fixed appliance was debonded and a multi-stranded stainless steel lingual retainer (0.016”) was bonded from the upper right to upper left first premolars to provide permanent retention.
Consideration was given to gingival grafting to manage the recession in the upper labial segment. However, the patient was reluctant to undergo further treatment as he was satisfied with the outcome.
Results
The post-treatment photographs indicated Class I incisor, molar and canine relationships bilaterally with corrected overbite and overjet. The pathological migration, traumatic occlusion, tooth mobility and diastema between the maxillary anteriors were eliminated. A post-treatment orthopantogram indicated the maintenance of sufficient bone support with no signs of significant root resorption (Figure 5a, b).
Figure 5.
(a, b) Post-treatment views and radiograph showing the corrected overbite and overjet, improved periodontal condition and dental aesthetics.
One year post-retention, the records indicated reduction of probing depth, no bleeding on probing, improvement in gingival margin relationship, maintenance of the bone level and stability of the final results (Figure 6a, b).
Figure 6.
(a, b) One year post-retention view and radiograph showing further improvement in the periodontal condition with no significant change in the occlusion.
Discussion
This paper describes adjunctive orthodontic treatment in an adult patient with severe periodontitis accompanied by marginal bone loss and pathological migration of the upper right anterior teeth.
Pathological migration is defined as a change in tooth position resulting from disruption of the forces that maintain the teeth in a normal position, with reference to the skull.6 The degree of migration will differ from tooth to tooth, according to the periodontal destruction and the forces acting on the single tooth. Secondary occlusal trauma resulting from pathological migration may further deteriorate the already compromised periodontium, as seen in the case presented here.
Intrusive movement has been recommended in cases of pathologic migration, to re-align the teeth and improve clinical crown length and marginal bone levels.7 Melsen et al concluded that intrusion of incisors in adult patients with marginal bone loss offers a beneficial effect on the periodontium at the clinical and radiographic level.5 Histological studies suggest that a new cementum and collagen attachment are formed after orthodontic intrusion if good oral hygiene is maintained.8,9 It has been reported that gingival recession improves after intrusion of a tooth.10,11,12
In the case presented here, intrusion of the elongated upper anterior teeth not only reduced the potential trauma to these teeth, but also improved the gingival relationships.
In the first stage of treatment, a modified orthodontic technique was employed where a periodontal splint was used in conjunction with a micro-implant to deliver a predictable force to intrude the upper right maxillary anterior teeth. A periodontal splint also allowed easier access to the teeth for oral hygiene purposes, which was crucial in this periodontally compromised case. During the second stage of treatment, a fixed orthodontic appliance was used to level and align, correct the incisor inclinations and close spaces in the upper arch.
In periodontally compromised teeth, the loss of alveolar bone results in the centre of resistance of the involved teeth moving apically Therefore, light controlled forces are important to minimize further attachment loss, tooth tipping and root resorption.7 The best results are obtained when tooth intrusion is performed with light forces (5–15 grams per tooth) and the line of action of the force passes close to the centre of resistance.5 The interval of orthodontic force activation should also be longer, because periodontal tissue remodelling is likely to take longer than in patients with healthy periodontal tissues. Therefore, in the present case, 15 grams (5 gram/tooth) of intrusive force was applied to intrude the splinted teeth using elastic thread between the splint and a micro-implant in the lateral incisor/canine region.
Knowledge concerning location of centre of resistance of various units of maxillary anterior dentition is necessary for vertical translation of teeth. Placement of micro-implants between lateral incisor and canine bilaterally at the level of attached gingiva has been recommended as the most suitable site for en masse intrusion of the maxillary anterior teeth.13,14 Therefore, we had placed the micro-implant between the apical third root length of the upper right lateral incisor and canine and used light force (5 gram/per tooth) so that the line of force application passed close to the anticipated centre of resistance of the upper right anterior dental segment, which minimized their proclination during the intrusion.
The design of the appliance in periodontally compromised cases will depend on a number of factors, such as the number of teeth to be moved, the availability of anchorage, and the desired direction and magnitude of tooth movement. Obtaining adequate anchorage for orthodontic tooth movement is frequently a major problem in partially dentate adult patients as there is reduced alveolar bone support. Also, in patients with severe periodontal involvement, there is the potential for further periodontal breakdown and tooth loss during treatment.15
In the case presented here, generalized bone loss was observed, particularly around the splinted teeth, therefore a micro-implant was used as an anchorage source to limit the use of the compromised adjacent teeth for anchorage purposes and minimal force was applied to intrude the teeth.
Dentition with severe bone loss shows a higher tendency for relapse after active orthodontic treatment.16 Permanent retention is often part of the overall treatment plan for these patients.17 Therefore, in this case, a multi-stranded stainless steel lingual retainer was bonded in the upper arch to achieve stable retention.
Conclusion
Orthodontic treatment in an adult patient with a compromised periodontium may restore the function and aesthetics provided physiologic light continuous forces are used, periodontal inflammation is controlled and meticulous oral hygiene is maintained throughout active therapy.