Abstract
CPD/Clinical Relevance: The reader will learn an alternative method for correcting anterior crossbites.
From Volume 17, Issue 2, April 2024 | Pages 80-81
CPD/Clinical Relevance: The reader will learn an alternative method for correcting anterior crossbites.
Anterior crossbites are a common feature seen in the mixed dentition and are reported in 7–10% of the UK population.1 Causes of anterior crossbite can be dental, or a reflection of an underlying Class 3 skeletal relationship.
Anterior crossbites can cause gingival recession to the lower incisors when the teeth are pushed labially out of the alveolar bone, and attrition to the incisal edges or labial surface of the upper incisors.2 The main patient concern is the appearance of a ‘stuck behind tooth’.
There are several appliance treatment options for anterior crossbites. The traditional approaches are either using an upper removable appliance with palatal springs, or a fixed appliance with 2 x 4 design. Treatment time has been demonstrated to take on average 6.9 months for removable and 5.5 months for fixed appliances.3 Disadvantages of a removable appliance include difficulty with speech during the initial settling in period. They also rely on good compliance.
Use of a fixed appliance can come with the traditional orthodontic risks, and can only be used in patients with excellent oral hygiene. This Trick of the trade outlines a different method that does not require an appliance, demands less patient compliance, and is more cost effective.
This method involves the use of composite incisal edge build-up to the most severely affected tooth in cross bite, opening the occlusion, 2–3 mm extra height is typically sufficient. The patient is then instructed to close within the retruded arc of closure rather than displace further forward in an unnatural and probably uncomfortable position. GoTo Paste (Reliance Orthodontic Products) is recommended; however, any composite or resin-modified GIC would be suitable. GoTo Paste has a clear, see-through appearance, which makes its later removal easier because the incisal edge can be seen underneath and there is less risk of damaging the enamel. Its appearance is also preferable because an opaque composite can give the appearance of a long tooth. The build-up should be kept at tooth thickness and preferably tapered palatally, to help guide the lower incisors behind it on mouth closure. A review appointment should be made at 1 month. However, most will correct within a couple of weeks, when the composite can be carefully removed with a slow speed debonding bur. If further correction is needed, the build-up can be added to. Care should be taken in using this method on teeth with prominent mamelons as composite removal could be difficult.
Patients should be warned that their bite may feel a little restricted, and the tooth could feel tender. Similar to fixed appliances, patients should be advised to take care with hard food and to return as soon as possible if the build-up breaks off.
This technique is suitable for patients with a Class 1 or mild 3 relationship, uncrowded or mildly crowded dentition and an anterior displacement. When first trying this method, it is advised to select patients with only one tooth in anterior crossbite. If there is crowding present or little overbite, then it is unlikely to be effective.
The merits of this method are:
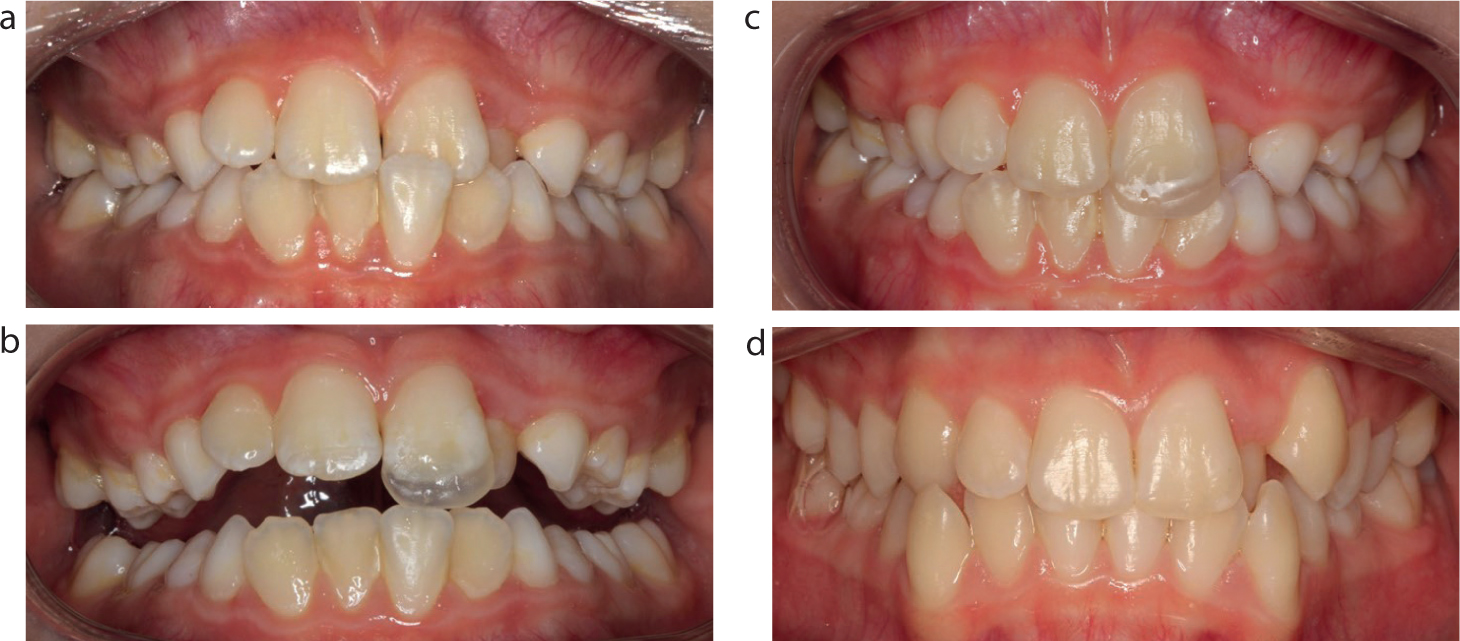
It is an ideal method for patients who may struggle to wear a removable appliance. Feedback from patients and parents has been positive, prompting this report. It is hoped that the case illustrations (Figures 1–3) will provide an alternative option to add to the armamentarium for treating anterior tooth crossbites.