Iida S, Matsuya T Paediatric maxillofacial fractures: their aetiological characters and fracture patterns. J Craniomaxillofac Surg. 2002; 30:237-241 https://doi.org/10.1054/jcms.2002.0295
Atilgan S, Erol B, Yaman F Mandibular fractures: a comparative analysis between young and adult patients in the southeast region of Turkey. J Appl Oral Sci. 2010; 18:17-22 https://doi.org/10.1590/s1678-77572010000100005
Posnick JC, Goldstein JA Surgical management of temporomandibular joint ankylosis in the pediatric population. Plast Reconstr Surg. 1993; 91:791-798 https://doi.org/10.1097/00006534-199304001-00006
Loukota RA, Abdel-Galil K Condylar fractures, 3rd edn.. In: Brennan PA, Schliephake H, Ghali GE, Cascarinin L London: Elsevier; 2017
Moss ML The primacy of functional matrices in orofacial growth. Dent Pract Dent Rec. 1968; 19:65-73
Lund K Mandibular growth and remodelling processes after condylar fracture. A longitudinal roentgencephalometric study. Acta Odontol Scand Suppl. 1974; 32:3-117
Stone N, Corneman A, Sandre AR Treatment delay impact on open reduction internal fixation of mandibular fractures: a systematic review. Plast Reconstr Surg Glob Open. 2018; 6 https://doi.org/10.1097/GOX.0000000000001829
Karan A, Kedarnath NS, Reddy GS Condylar fractures: surgical versus conservative management. Ann Maxillofac Surg. 2019; 9:15-22 https://doi.org/10.4103/ams.ams_157_17
Morisada MV, Tollefson TT, Said M Pediatric mandible fractures: mechanism, pattern of injury, fracture characteristics, and management by age. Facial Plast Surg Aesthet Med. 2022; 24:375-381 https://doi.org/10.1089/fpsam.2022.0031
Kaban LB, Mulliken JB, Murray JE Facial fractures in children: an analysis of 122 fractures in 109 patients. Plast Reconstr Surg. 1977; 59:15-20 https://doi.org/10.1097/00006534-197701000-00002
Khattak YR, Sardar T, Iqbal A Treatment of pediatric bilateral condylar fractures: a comprehensive analysis. J Stomatol Oral Maxillofac Surg. 2023; 124:(1S) https://doi.org/10.1016/j.jormas.2022.11.015
Stähli C, Eliades T, Papageorgiou SN Functional appliance treatment for mandibular fractures: a systematic review with meta-analyses. J Oral Rehabil. 2021; 48:945-954 https://doi.org/10.1111/joor.13178
Zhao YM, Yang J, Bai RC A retrospective study of using removable occlusal splint in the treatment of condylar fracture in children. J Craniomaxillofac Surg. 2014; 42:1078-1082 https://doi.org/10.1016/j.jcms.2012.07.010
Hovinga J, Boering G, Stegenga B Longterm results of nonsurgical management of condylar fractures in children. Int J Oral Maxillofac Surg. 1999; 28:429-440
Gupta S, Verma R, Sahu N Various approaches for the management of mandibular fracture in pediatric patients: a case series. J Adv Clin Res Insights. 2022; 9:16-19 https://doi.org/10.15713/ins.jcri.355
Polizzi A, Ronsivalle V, Lo Giudice A Orthodontic approaches in the management of mandibular fractures: a scoping review. Children (Basel). 2023; 10 https://doi.org/10.3390/children10030605
Sandier J, Lindsay S, Murray A Orthodontic appliances for reduction and fixation of a mandibular fracture: a case report. Dent Update. 2007; 34:239-242 https://doi.org/10.12968/denu.2007.34.4.239
Mandibular fractures in children are different to those in adults. Greenstick fractures are more commonplace, and displacement less frequently encountered. They are mostly treated conservatively; however, if the occlusion is altered, then reduction will be required. Closed reduction is normally favoured in children because open surgical reduction and internal fixation may impair future growth. Closed reduction is often carried out with arch bars or splints. These may be traumatic and painful for the child. This case report describes the case of a 12-year-old boy who presented with bilateral condylar fractures with displacement and deranged occlusion. Minimal fixed appliance treatment was used to reduce the fractures and restore him to his pre-injury occlusion.
CPD/Clinical Relevance: Minimal orthodontic treatment can be used to reduce a bilateral condylar fracture with displacement in paediatric mandibular fractures.
Article
Fractures of the mandible are the most frequent facial skeletal injury as a result of facial trauma in children.1 In paediatric mandibular fractures, the condyle is the most common fracture site, followed by the symphysis/parasymphysis, the body, and then the angle.2,3
Condylar fractures mostly occur via blunt force to the anterior mandible transmitted to the condylar region. Involvement of the temporomandibular joint (TMJ) in the fracture, or excessive immobilization in treatment, may cause altered occlusion and/or ankylosis of the joint.4
The condylar cartilage is not a primary growth centre for the mandible, but still has an adaptive response.5 Therefore, trauma to the condylar region can also result in underdevelopment of the mandible. It is estimated that 75% of children who undergo a condylar fracture have normal mandibular growth.6
Derangement of occlusion is the most important factor when deciding whether the fracture requires intervention.7 The aims of treatment are to achieve normal opening and movement, pre-treatment occlusion, and facial symmetry.
In adults, open reduction and internal fixation (ORIF) of osteosynthesis plates has become the gold standard in treatment of mandibular fractures.8 However, condylar fractures are normally treated via closed reduction and immobilization due to the surgical risk of damage to the facial nerve due to its anatomical position.9 Non-surgical reduction involves the use of elastic intermaxillary fixation (IMF) to produce a normal occlusion.10 This may be achieved with arch bars, intermaxillary fixation screws, splints, or bonded orthodontic brackets.
In children, the management differs with closed reduction being favoured because surgical intervention risks impairing skeletal growth or even harming the developing dentition.4,11 Young bone may become partially united by the fourth day, and become difficult to reduce by the seventh day, so fixation may be required as early as possible.12 Owing to the possible disruption in growth, the final result depends on the long-term effect on growth and not just the initial treatment.13
Most fractures of the body, symphysis, and angle in children are undisplaced owing to the flexibility of the mandible and tooth buds, which keep the fractured parts together. If reduction is required, the dentition is used to allow intermaxillary fixation. If teeth cannot be used, then gunning splints may be required.13
For condylar fractures, a non-chew diet and conservative management is normally sufficient. However, bilateral fractures with substantial displacement normally produce malocclusion with an open bite tendency. Different methods may be employed for IMF including arch bars, occlusal splints or orthodontic brackets. With orthodontic brackets, guiding elastics are then used to guide the mandible into the correct occlusion, and if the malocclusion persists, then open reduction must be considered.14 Functional appliances can be effective;15 however, achieving the ideal occlusion may be challenging. A removable semi-hard occlusal splint worn for 1–3 months until restoration of occlusal relationship is another effective option.16
In this case report, we demonstrate the use of fixed appliances to provide intermaxillary fixation in a case of bilateral condylar fracture in a child.
Case report
A fit and well 12-year-old boy presented to the accident and emergency department (A&E) after falling off his bike. He complained of discomfort to his TMJs and a deranged occlusion. He sustained a laceration to his chin, which was sutured in A&E. He had a Class III malocclusion with a reverse overjet, and limited movement in opening and lateral excursions (Figure 1). Previous family photographs showed that he originally had a Class I occlusion with a normal overbite and overjet.
Figure 1. Intra-oral views 3 days after the trauma.
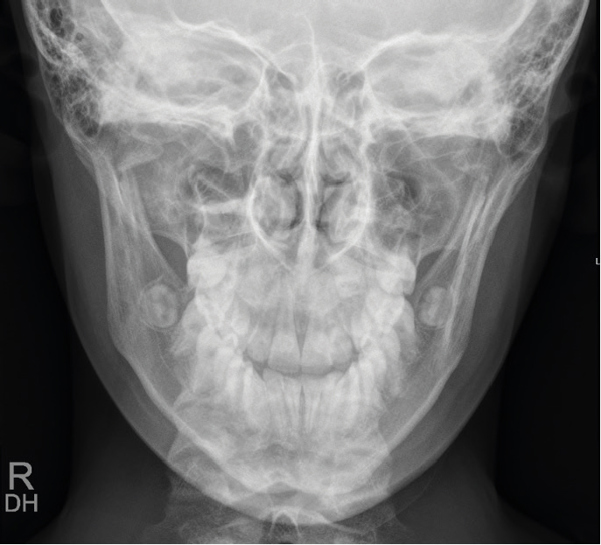
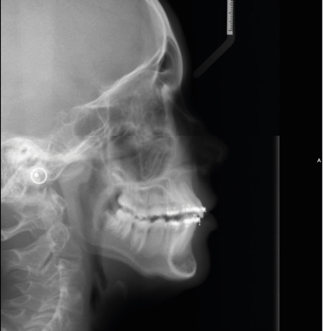
A dental panoramic tomograph (DPT) and postero-anterior (PA) mandible radiograph were taken. These confirmed bilateral condylar fractures (Figures 2 and 3). A lateral cephalogram was also taken to record the altered occlusion (Figure 4). This showed a Class III incisor relationship with lateral open bites.
Figure 2. DPT showing the bilateral condylar fracture.Figure 3. PA mandible confirming bilateral condylar fracture.Figure 4. Lateral cephalogram showing the altered occlusion.
Bilateral condylar fractures often produce an open bite as the ramus height is shortened.13 Interestingly, in this case, an edge-to-edge occlusion occurred with the mandible postured forward. The mandible may have displaced forward following the fracture.
Owing to the risks associated with the facial nerve from open reduction and internal fixation to the condylar area, as well as the potential negative effects on future growth from surgical correction, the maxillofacial team at the Royal Surrey Foundation Trust requested that the patient be seen jointly with the orthodontic team for a conservative intermaxillary fixation approach.
Orthodontic brackets were bonded from first premolar to first premolar in each arch. The appliance was not extended back further owing to discomfort on opening. Canine brackets were used on the first premolars and lower central incisors to add extra points of application for elastics. It was important to bond the brackets in a passive way so that the slots would line up. Changing tooth position was not the aim. The brackets and wires were solely to facilitate application of the elastic force to correct the occlusion. 0.018” stainless steel wires were passively ligated in the upper and lower arches. Some brackets could only be partially ligated to prevent unwanted tooth movement. Medium force elastics (¼” diameter, 3.5 oz) were used bilaterally as a Class III vector from the lower central incisors to the upper first premolars to give the greatest range of activation. There was an immediate improvement in the occlusion chairside (Figure 5).
Figure 5. Occlusion immediately after placing Class III elastic vector.
There was some discomfort during the bond up, but the patient coped well. Normal oral analgesia that would be advised for orthodontic pain, paracetamol and/or ibuprofen, was advised to be taken as required. The patient and parents were instructed in how to change the elastics and the child was advised on a soft non-chew diet and to avoid sport or exercise that could risk further trauma or hinder healing.
The patient was reviewed 1 week later and the occlusion was satisfactorily corrected to Class I with a normal overbite and overjet. He was subsequently reviewed 2 weeks later. The DPT and lateral cephalogram were repeated (Figures 6 and 7). The lateral cephalogram showed the corrected occlusion. Although the occlusion was corrected, the DPT showed that the condylar height was still shortened. The mandible had been guided back into centric occlusion, but there may have still been some vertical overlap between the fractured condyle and ramus causing the appearance on the radiograph.
Figure 6. DPT following 3 weeks of IMF.Figure 7. Lateral cephalogram showing correction of Class III malocclusion.
Following discussion with maxillofacial colleagues, the fixed appliances were removed (Figure 8). The patient followed conservative advice regarding diet and sport activity for a further 3 weeks, until 6 weeks post injury.
Figure 8. Debond photos.
This method was not without risk. Undesirable tooth movement was a possibility, although the brackets were bonded to allow passive ligation of the wire and prevent unwanted tooth movement. The patient may require further orthodontic detailing when he is fully in the permanent dentition.
Discussion
The long-term regeneration and growth of the condyle following the trauma is what determines whether facial asymmetry occurs due to the fracture. In a retrospective review of non-surgically treated condylar fractures, high condylar fractures show better regeneration radiographically than low or intracapsular fractures.17
Paediatric mandibular fractures are different to adults. Usually, they are greenstick fractures, while displaced fractures are a rarer occurrence. They heal quickly, and even imperfectly reduced fractures have a good likelihood of healing correctly.18,19 As ORIF may disrupt growth, closed reduction is the method of choice for paediatric mandibular fractures.
Arch bars, IMF screws or occlusal splints fixed with circumferential wiring are normally provided by a maxillofacial surgeon. However, these approaches may add discomfort, impinge on mucosa and cause periodontal tissues, impair oral hygiene, risk enamel demineralization and the arch bars may be less retentive on conical deciduous teeth.20 Orthodontics offers a less invasive approach. It is particularly useful in children and there are reports of it being used in adults for minimally displaced mandibular fractures.21
Although, an orthodontic department or a dentist skilled in orthodontics is not always easily accessible to provide the treatment, in the UK many orthodontic departments work closely with a maxillofacial department. Therefore, this is a treatment modality that should be considered for paediatric mandibular fractures.