Björk A, Skieller V Normal and abnormal growth of the mandible. A synthesis of longitudinal cephalometric implant studies over a period of 25 years. Eur J Orthod. 1983; 5:1-46 https://doi.org/10.1093/ejo/5.1.1
Leslie LR, Southard TE, Southard KA Prediction of mandibular growth rotation: assessment of the Skieller, Björk and Linde-Hansen method. Am J Orthod Dentofacial Orthop. 1998; 114:659-667 https://doi.org/10.1016/s0889-5406(98)70198-2
Hunt NP, Cunningham SJ The influence of orthognathic surgery on occlusal force in patients with vertical facial deformities. Int J Oral Maxillofac Surg. 1997; 26:87-91 https://doi.org/10.1016/s0901-5027(05)80633-2
Hunt N, Shah R, Sinanan A, Lewis M Northcroft Memorial Lecture 2005. Muscling in on malocclusions: Current concepts on the role of muscles in the aetiology and treatment of malocclusion. J Orthod. 2006; 33:187-197 https://doi.org/10.1179/146531205225021660
Naini FB, Gill DS, Sharma A, Tredwin C The Aetiology, Diagnosis and Management of Deep Overbite. Dent Update. 2006; 33(6):334-336 https://doi.org/10.12968/denu.2006.33.6.326
Ng J, Major PW, Heo G, Flores-Mir C True incisor intrusion attained during orthodontic treatment: A systematic review and meta-analysis. Am J Orthod Dentofacial Orthop. 2005; 128:212-219 https://doi.org/10.1016/j.ajodo.2004.04.025
Burstone CJ The mechanics of the segmented arch techniques. Angle Orthod. 1966; 36:99-120
Almuzian M, Alharbi F, Lai-King Chung L, McIntyre GT Transpalatal, Nance and lingual arch appliances: Clinical tips and applications. Orthod Update. 2015; 8:92-100 https://doi.org/10.12968/ortu.2015.8.3.92
Naish HJ, Dunbar C, Atack NE The control of unwanted tooth movement - an overview of orthodontic anchorage. Orthod Update. 2015; 8:42-54 https://doi.org/10.12968/ortu.2015.8.2.42
Cousley R The Orthodontic Mini-implant Clinical Handbook. Wiley-Blackwell. 2013;
Motoyoshi M, Matsuoka M, Shimizu N Application of orthodontic mini-implants in adolescents. Int J Oral Maxillofac Surg. 2007; 36:695-699 https://doi.org/10.1016/j.ijom.2007.03.009
Deguchi T, Murakam T, Kuroda S, Yabuuchi T Comparison of the intrusion effects on the maxillary incisors between implant anchorage and J-hook headgear. AJODO. 2008; 133:654-660
Khosravi R, Cohanim B, Hujoel P Management of overbite with the Invisalign appliance. Am J Orthod Dentofacial Orthop. 2017; 151:691-699
Blundell H, Weir T, Kerr B Predicatability of overbite control with the Invisalign appliance. Am J Orthod Dentofacial Orthop. 2021; 160:725-731
Ireland AJ, Songra G, Clover M Effect of gender and Frankfort mandibular plane angle on orthodontic space closure: a randomized controlled trial. Orthod Craniofac Res. 2016; 19(2):74-82
Beddis HP, Durey K, Alhilou A, Chan MFWY The restorative management of the deep overbite. Br Dent J. 2014; 217(9):509-515
Littlewood SJ, Millett DT, Doubleday B, Bearn DR, Worthington HV Retention procedures for stabilising tooth position after treatment with orthodontic braces. Cochrane Database Syst Rev. 2016; https://doi.org/10.1002/14651858.CD002283.pub4.
Huang G, Bates S, Ehlert A, Whiting D Stability of deep-bite correction: A systematic review. J World Fed Orthod. 2012; 1:e89-e86
Skeletal discrepancies. Part 1: assessment, aetiology, and management of low angle cases Jenifer L Jopson Peter Fowler Dental Update 2024 16:3, 707-709.
This is the first article in a three-part series considering skeletal discrepancies in the vertical and transverse dimensions. Discrepancies in the vertical dimension are a relatively common finding, presenting challenges for the orthodontist, in terms of treatment planning, management and relapse.
CPD/Clinical Relevance: This article aims to increase awareness of the assessment, aetiology and management of patients presenting with a reduced Frankfort/maxillary mandibular planes angle and reduced anterior lower face height commonly described as ‘low angle’.
Article
Diagnosing discrepancies in the vertical dimension is vital to understanding how skeletal, dental and soft tissue factors contribute to the development of a malocclusion. This article provides an overview of the assessment of the vertical dimension and discusses the aetiology and management of patients presenting with a reduced Frankfort/maxillary mandibular planes angle (F/MMPA) and anterior lower face height (ALFH).
Definition of low angle and prevalence
The definition of ‘low angle’ in orthodontics is a decreased FMPA more than one standard deviation below the average of 27° (such as an FMPA <22°).
A low angle is associated with decreased vertical facial proportions and may be associated with a forward growth rotation of the mandible. Other terms used to describe a low angle include hypodivergent, brachyfacial and short face.
There is currently limited evidence available regarding the prevalence of patients with a ‘short face’.
Assessment of the vertical dimension
Frontal examination
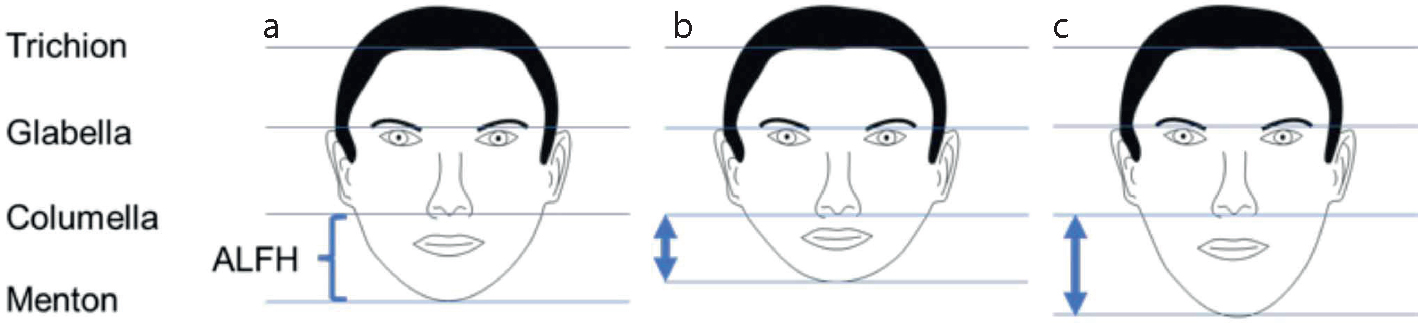
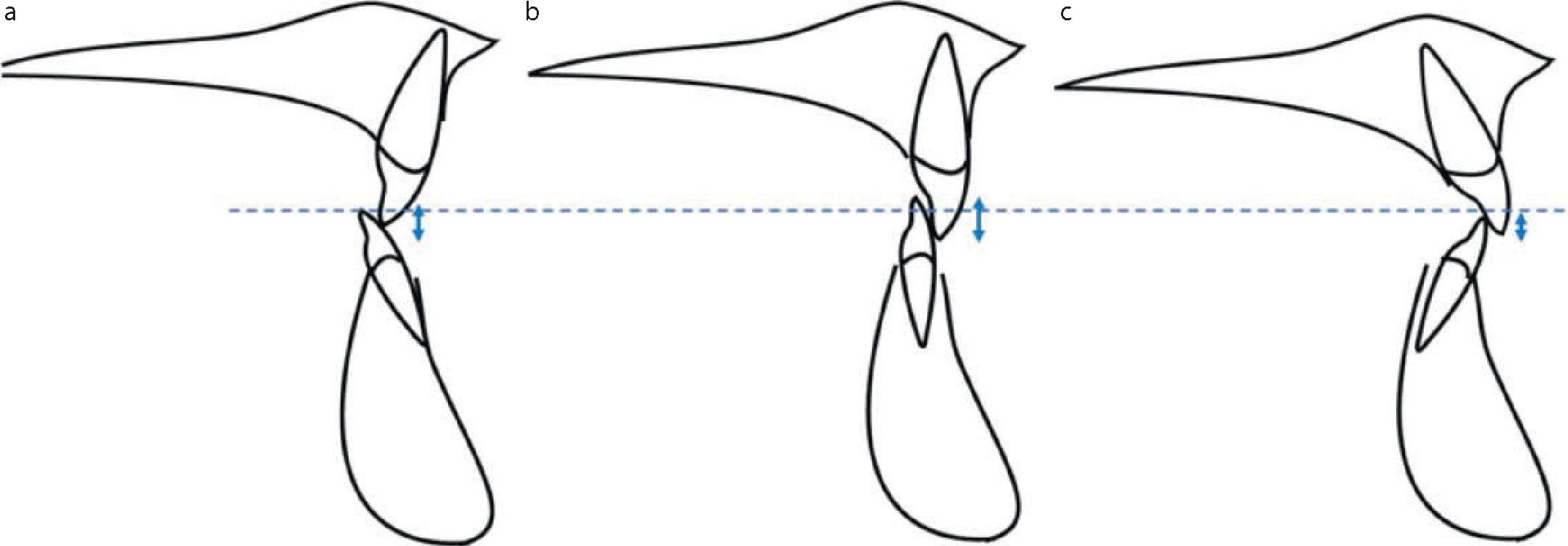
During a frontal examination, the face height can be divided into thirds, with each third being roughly equal in length (Figure 1). The upper third is measured from trichion to glabella. The middle third, usually described as the anterior upper face height (AUFH), is measured from glabella to columella. The ALFH is measured from columella to soft tissue menton. The AUFH and ALFH may be equal, increased or decreased with respect to each other.
Figure 1. (a) Average, (b) reduced and (c) increased anterior lower face height.
Profile examination
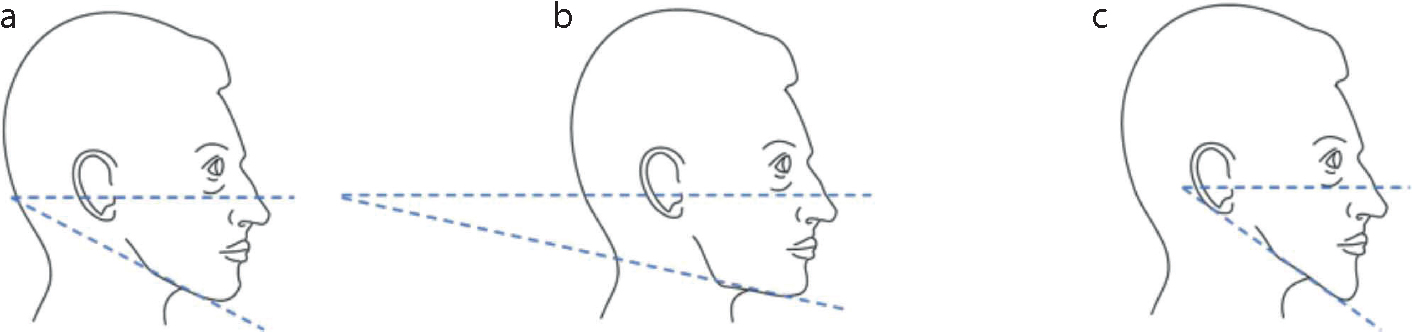
In profile, the vertical skeletal dimension can be assessed using the same linear measures as previously described, but also using angular measures. The most common angular measure is the FMPA. This angle, which represents the ratio of the ALFH to the posterior lower face height (PLFH), is assessed by visualizing where the projected lines of the mandibular plane and the Frankfort plane intersect relative to the occiput. The Frankfort plane is a line connecting the lower border of the orbit to the upper border of the external auditory meatus and is easily visualized clinically. An average FMPA is identified where the two lines intercept at the occiput. If the lines intercept posterior to the occiput, the patient is reported to have a reduced FMPA or ‘low angle’. Conversely, if the lines intercept anterior to the occiput it is an increased FMPA or ‘high angle’ (Figure 2).
On a lateral cephalometric radiograph, the AUFH and ALFH are measured from perpendiculars constructed to the maxillary plane, to nasion and to menton, respectively. The AUFH should comprise 45%, and ALFH 55%, of the total face height.
The maxillary plane, constructed by joining the points of the anterior nasal spine to the posterior nasal spine, is used instead of the Frankfort plane because landmark identification on the cephalometric radiograph is easier. The angle created by the intersection of the maxillary plane with the mandibular plane (constructed by joining the two points, menton and gonion) is known as the maxillary mandibular planes angle (MMPA) and, on average, also measures 27° ± 5°.
It is important to note that a patient can present with a reduced ALFH, but still have an average FMPA/MMPA angle. This is because the FMPA/MMPA is a measure of the ratio of anterior lower face height to posterior lower face height.
Aetiology of skeletal vertical discrepancies
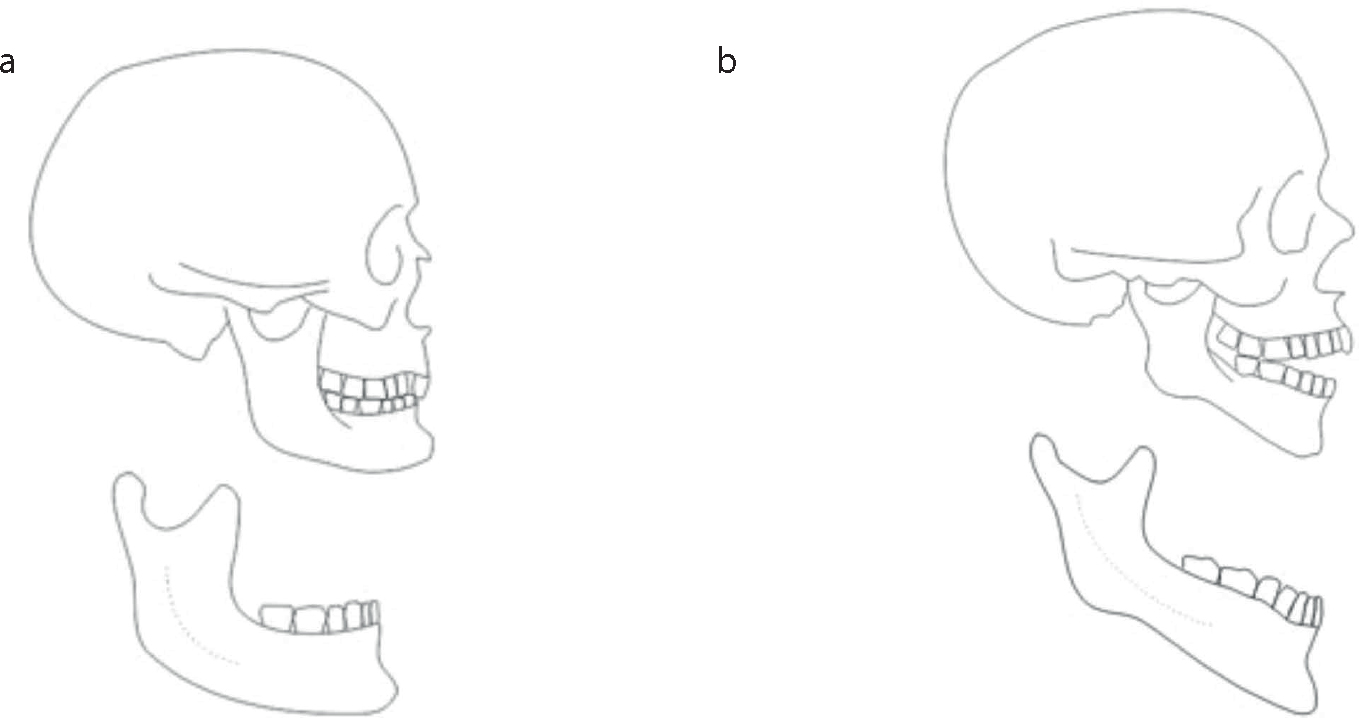
Longitudinal implant studies, carried out primarily by Björk et al during the 1960s, demonstrated that during growth, both the maxilla and mandible may be subjected to internal and external rotational effects. These growth rotations have the most noticeable impact on the mandible, which rotates either around the condyle, the lower incisal edges or within the body of the mandible itself.1 These rotations are a result of differential growth at key sites, such as the condyles or the soft tissues.2 Growth rotations are classified as either ‘forward’ (posterior facial growth being greater than anterior facial growth) or ‘backward’ (anterior growth being greater than posterior growth) (Figure 3) with 80% of the population thought to have a forward mandibular rotation and 20% a backward rotation. An excessive forward growth rotation is typically characterized by both a low MMPA and a reduced ALFH.
Björk described seven radiographic structural signs that may be indicative of a growth rotation (Table 1), although the reliability of this method has been questioned.3,4
Table 1. Structural signs of forward and backward growth rotations.
Forward growth rotation
Backward growth rotation
1. Forward inclination of the condylar head
1. Backward inclination of the condylar head
2. Increased curvature of the mandibular canal
2. Reduced curvature of the mandibular canal
3. Flat lower border of the mandible
3. Concavity at the border of the mandible, such as the antegonial notch
4. Forward positioning of the mandibular symphysis
4. Backward positioning of the mandibular symphysis
5. Increased interincisal angle
5. Reduced interincisal angle
6. Increased intermolar angle
6. Reduced intermolar angle
7. Reduced anterior lower face height
7. Increased anterior lower face height
The relationship between masticatory muscles and low angle cases
Research has demonstrated that patients with reduced vertical dimensions generate greater occlusal forces than their counterparts with normal or increased vertical dimensions.5 It is uncertain whether it is the form and function of the masticatory muscles that influence the malocclusion or vice versa.6
Features commonly associated with low angle cases
In addition to the features described by Björk3 (Table 1), it is common to observe other skeletal, soft tissue and dental features in patients presenting with a low angle (Table 2).
Table 2. Features commonly observed in low angle cases.
Factor
Features
Skeletal
Reduced Frankfort/maxillary mandibular planes angle and reduced or normal anterior lower face height Square type face
Soft tissue
Hypertrophic masseter muscles Deep labio-mental fold ‘Strap-like’ lower lip High resting lower lip Gingival trauma labial to the lower incisors and palatal to the upper incisors
Dental
Increased overbite Increased curve of Spee Increased interincisal angle Overeruption of upper and lower incisors
Considerations for treatment planning in a low angle case
Questions to consider when planning treatment for a patient with a low angle and an increased overbite (Figure 4) are shown in Table 3.
Figure 4. ‘Low angle’ patient with the typical features of reduced Frankfort mandibular plane, reduced anterior lower face height, deep labiomental fold, increased interincisal angle and increased overbite
Table 3. Factors to consider during treatment planning of a low angle case.
Is the overbite acceptable or does it require correction as part of the orthodontic treatment?
Is the overbite caused by relative overeruption of the lower incisors, overeruption of the upper incisors, or both?
Is there an anteroposterior skeletal discrepancy that requires treatment?
Is the patient still growing?
Can the overbite be treated with orthodontic camouflage or growth modification, or is an orthognathic surgical approach required?
What is the gingival phenotype, if lower incisor proclination is planned?
What are the space requirements to reduce the overbite?
What is the likely stability of the overbite following correction?
What is the likely cooperation of the patient?
Tooth movements associated with the correction of the overbite
An increased overbite can be reduced orthodontically using several different methods, including molar and premolar extrusion/differential eruption, lower and upper incisor intrusion, or incisor proclination.7
Posterior extrusion/eruption
Overbite reduction by posterior extrusion/ differential eruption is possible with posterior tooth eruption relative to the incisor teeth, creating the ‘wedge effect’, which increases the MMPA and ALFH. Although this increase in MMPA and ALFH may be desirable if the patient has a reduced ALFH, the effective change in the vertical skeletal relationship is likely to be transient.7 In the growing patient, the MMPA is likely to return to the pre-treatment value because the face continues to grow. In the adult patient, in the absence of growth, posterior extrusion/differential eruption may take much longer to occur. If the overbite reduction is to be maintained, the incisors must be intruded, particularly in the adult patient.
Intrusion of the incisors
Reducing an overbite by true intrusion of the incisors theoretically has no effect on the MMPA or ALFH. It can be difficult to achieve, and certainly requires complex fixed appliance intrusion mechanics, as it is necessary for the incisors to intrude within a narrow alveolar trough and without contacting the cortical bone (Figure 5). If the incisor roots contact the cortical plate of bone (Figure 6), there is an increased likelihood that overbite reduction will instead be a result of molar extrusion.8 Absolute anchorage in the form of mini implants, in combination with fixed appliance mechanics, may improve the chances of achieving true incisor intrusion.
Figure 5. Incisors intruding within a narrow alveolar trough.Figure 6. True incisor intrusion hindered by roots hitting the cortical plate.
Proclination of the incisors
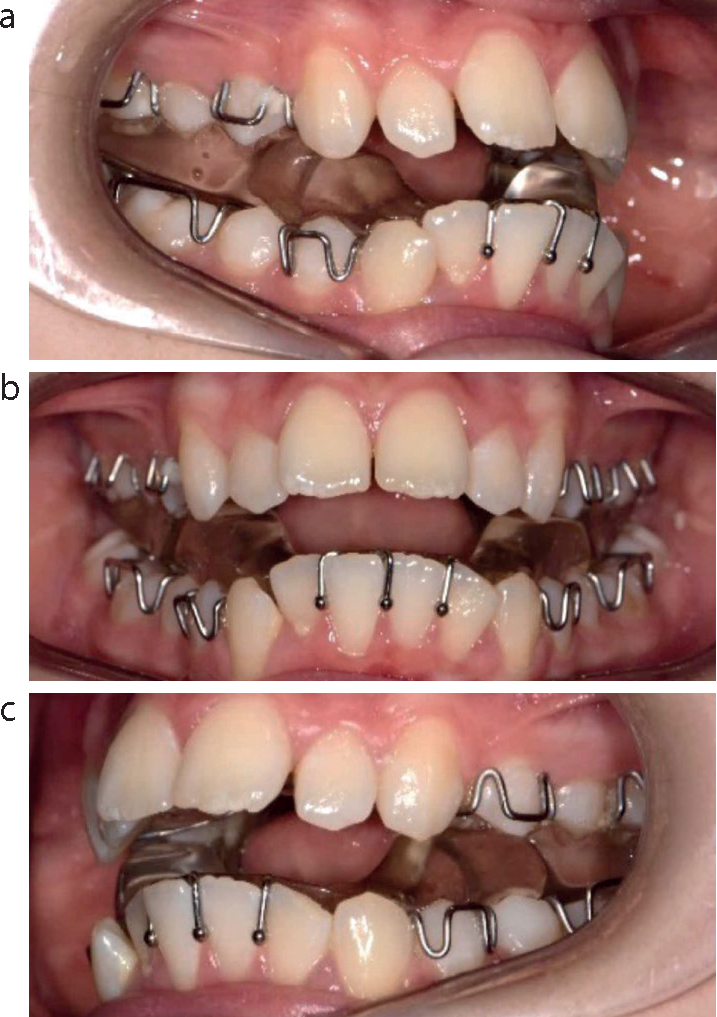
Another method to reduce the overbite is through incisor proclination. It has been stated that for every 5° of lower incisor proclination, the overbite reduces by 1 mm.9 Although considered an unstable movement, proclination of the lower incisors is a common method of overbite reduction.10 However, attention must be paid to the supporting soft tissues, ie the gingival phenotype, in order to avoid adverse effects such as recession, as the teeth tip labially.7 For very retroclined incisor teeth, initially the overbite will increase when proclination of the incisors in undertaken (Figure 7).
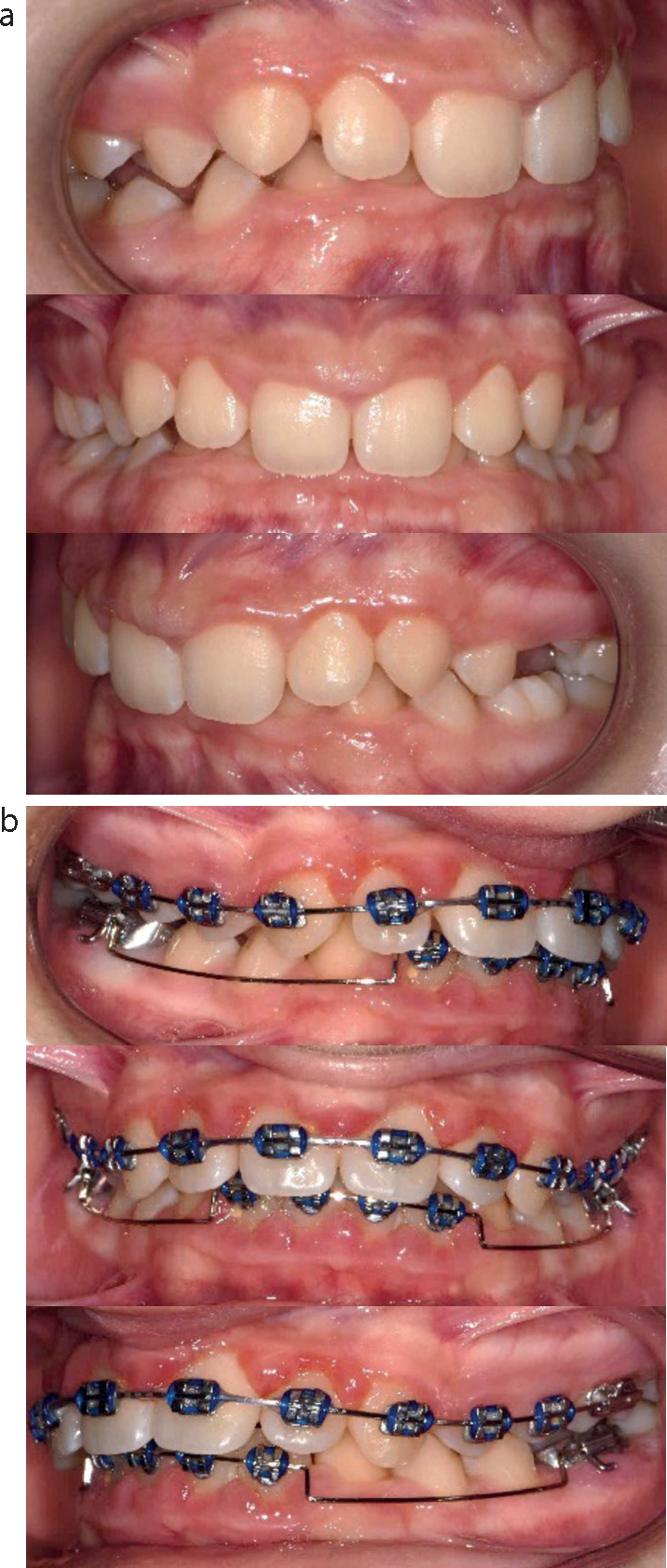
Figure 7. Overbite reduction through incisor proclination. (a) Start: increased overbite associated with severely retroclined upper and lower incisors. (b) Mid-treatment during incisor proclination: overbite increases during treatment. (c) End of treatment: correction of overbite and interincisal angle.
Methods of overbite reduction
There are a number of methods available to the orthodontist to reduce the overbite, namely differential tooth eruption (molar/premolar extrusion), incisor intrusion or incisor proclination and these often occur in combination.
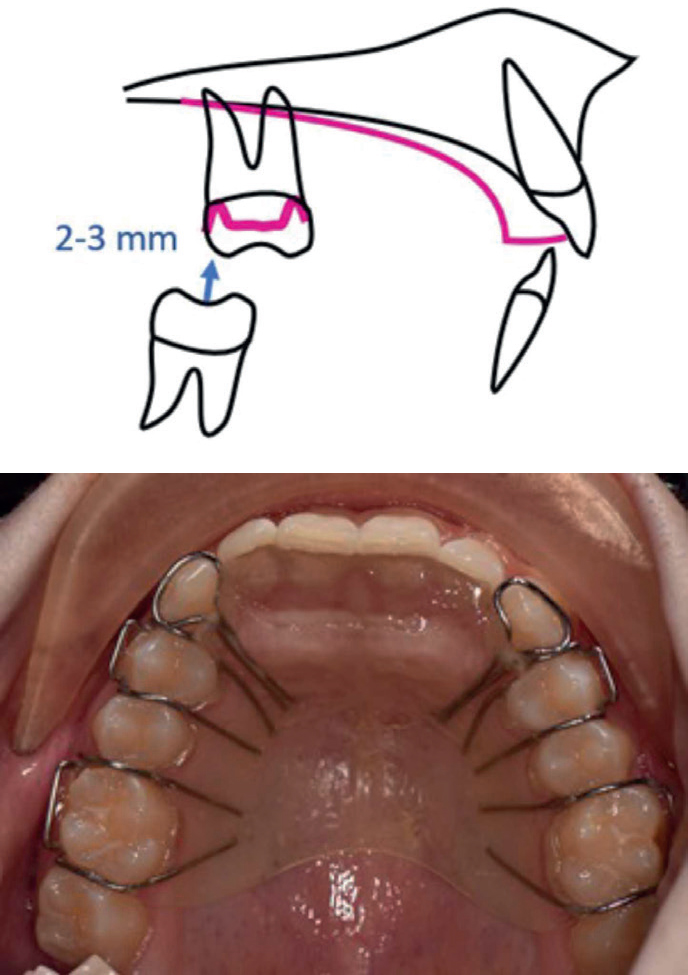
Upper removable appliance with a flat anterior bite plane
In a growing patient, an upper removable appliance with a flat anterior bite plane (FABP), which discludes the molars by 2–3 mm, has the effect of maintaining the position of the lower incisors and facilitating the differential eruption of the posterior teeth (Figure 8). Compensatory growth at the condyle may occur in the growing patient.
Figure 8. Use of an upper removable appliance with an anterior bite plane to correct the overbite.
Functional appliances
Functional appliances are commonly used to treat Class II division 1 or Class II division 2 incisor relationships in growing patients. As well as effecting a change in the antero-posterior skeletal and dento-alveolar relationships, they can be used to reduce the overbite.7
One-piece functional appliances, such as the medium opening activator or bionator (Figure 9), can be made with lower incisor capping, which mimics the action of a flat anterior bite plane, thereby allowing eruption of the posterior mandibular teeth while restraining the lower incisors. With a two-piece functional appliance, such as a modified Clark twin block (Figure 10), or a one-piece appliance where the acrylic overlying the buccal segment teeth is left untrimmed, the lower buccal segment teeth are initially prevented from erupting. During treatment, while maintaining the corrected overbite, the posterior acrylic can then be trimmed to allow the differential eruption of the posterior teeth.11
Figure 9. Bionator appliance with the acrylic trimmed away over the lower posterior teeth, allowing overbite correction by molar/premolar eruption while restraining the lower incisors.Figure 10. (a–c) Modified Clark twin block appliances. This design, with Adams cribs on the lower first permanent molars, does not initially allow lower posterior teeth to erupt.
Fixed appliances
A fixed appliance can be used to reduce an increased overbite either by molar extrusion, incisor intrusion, incisor proclination or a combination of all three.
Working archwires
Following initial alignment, larger dimension continuous archwires reduce the overbite by levelling an increased curve of Spee (COS) in the lower arch and increased reverse COS in the upper arch. In an unspaced upper or lower arch, levelling the COS will result in further proclination of the incisors as the arch length increases with relative premolar extrusion (Figure 11).
Figure 11. (a) Increased overbite at start of treatment. (b) Increased curve of Spee incorporated into upper continuous archwire. Lower utility intrusion arch.
Increase in arch length can be prevented by gaining space through extractions or interproximal reduction. In low angle cases with an increased overbite, lower arch extractions have the potential to complicate overbite reduction, by reducing the capability to procline the lower incisors. In addition, caution must be taken not to create excessive space, as residual space closure may lead to the retroclination of the lower incisors and a recurrence of the increased overbite.12 This may be due to an inadequate occlusal stop with the upper incisors at the end of treatment, as a result of a residual overjet, an increased interincisal angle, or both.
Once in larger stainless-steel wires, the addition of a reversed COS in the lower archwire and increased COS in the upper will accentuate the tooth movements otherwise achieved using a flat continuous archwire.
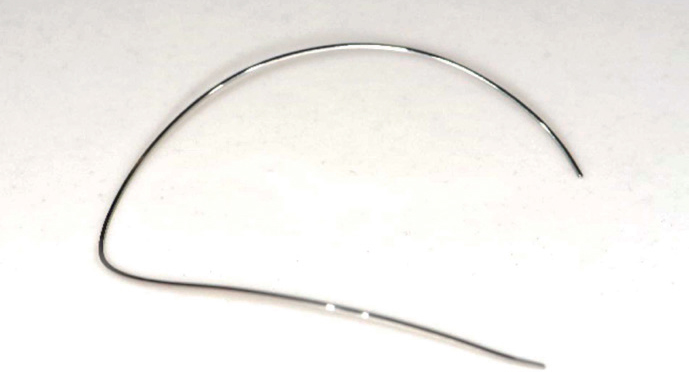
Nickel-titanium archwires with a preformed reversed COS (Figure 12) can be used to reduce an overbite, but lingual crown torque cannot be applied, meaning lower incisor proclination is much more likely. Regular monitoring is required owing to the unwanted side effects that these wires can have on the arch form, such as expansion in the premolar region or excessive lower incisor proclination.
Figure 12. Nickel–titanium archwire with a preformed reversed curve of Spee.
Segmental archwires
In adults, relying on relative molar extrusion mechanics alone may not be stable in the long term. Instead, absolute intrusion of the incisors can increase stability and is possible to achieve with segmental arch mechanics, including Ricketts’ utility arch and the Burstone intrusion arch.13,14 In a study of non-growing patients, it was reported that up to 1.5 mm maxillary and 1.9 mm mandibular incisor intrusion could be achieved using these mechanics.8 Such mechanics may be indicated in non-growing individuals with upper incisor excessive gingival show, where there is overeruption of the lower incisors, and where the reduced ALFH can be accepted.
Additional methods for reducing an overbite
Bonding the lower second molars
Incorporating lower second molars into fixed appliances (Figure 13) early in treatment aids overbite reduction by levelling the COS.
Figure 13. Use of lower fixed appliance, incorporating second molars.
Fixed anterior bite planes
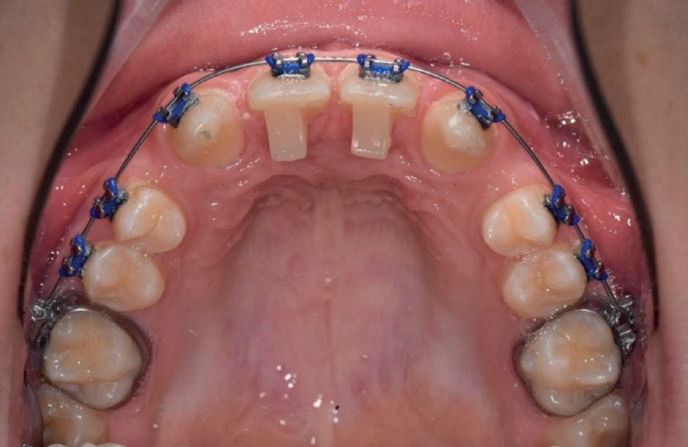
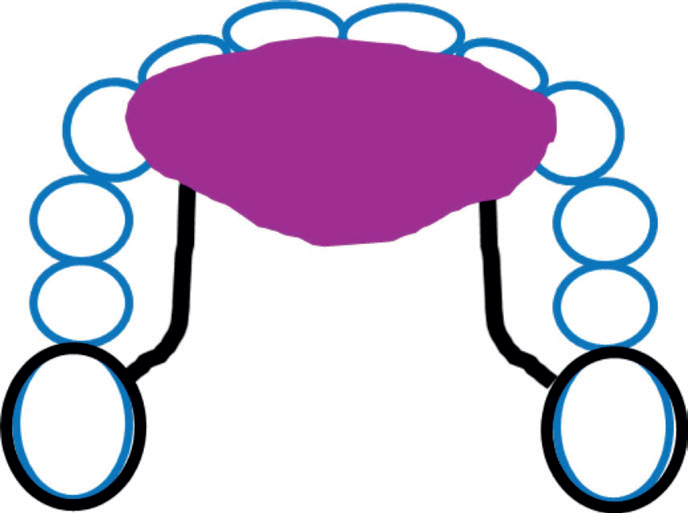
Fixed anterior bite planes are usually bonded to the palatal surfaces of the anterior teeth and are available in a variety of materials, including acrylic, metal, resin composite and glass ionomer cements. Fixed anterior bite planes (bite turbos) can be prefabricated or made at the chair side (Figure 14), but these are only effective if the overjef allows the lower incisors to contact the bite turbos.12 For patients with additional anchorage demands, a fixed anterior bite plane can be incorporated into a modified transpalatal arch (Figure 15).15 Potential disadvantages of this design include proclination of the upper incisors and increased risk of decalcification, or caries on the palatal aspect of the upper incisors.
Figure 14. Bite turbos on palatal surfaces of both upper central incisors, fabricated chairside.Figure 15. Fixed anterior bite plane incorporated into a modified transpalatal arch
Class II intermaxillary arch elastics
Class II elastics are worn from the mandibular molars to the maxillary anterior teeth, either to the maxillary archwire or directly to a tooth, and are effective in simultaneously reducing the overbite and overjet.16 Although they will extrude both the mandibular molars and maxillary incisors, overbite reduction will still occur. This is a result of the ‘wedge effect’, meaning that extrusion of the molar at the back of the mouth (or wedge) will have a greater effect on overbite than the same degree of maxillary incisor extrusion at the front of the mouth. Class II elastics can cause unwanted tooth movements, such as proclination of the lower incisors and maxillary incisor extrusion. This can be minimized with the incorporation of lower labial root torque to the archwire and an increased COS in the upper archwire respectively. Although these tooth movements may sometimes be unwanted, in many cases the effect of Class II elastics leading to lower incisor proclination may be planned in order to help overbite and overjet reduction.
Absolute anchorage
Absolute intrusion of the incisors can also be achieved with the use of temporary anchorage devices and is suited for adult patients with an increased overbite due to overeruption of teeth, increased gingival show and vertical maxillary excess.17 Many factors can influence the likely success of using mini-implants, but adolescents have an increased mini-implant failure rate compared to adults.18 Methods for overbite reduction using mini-implants are described in Table 4.
Table 4. Methods of overbite reduction using mini-implants.17
Direct anchorage
Labial/buccal implants are directly loaded to individual teeth or the archwire. Unwanted tooth movements involve changes to the labial crown torque of the upper incisors
Indirect anchorage
Using the reinforced anchorage of molar teeth to reduce the overbite with an intrusion archwire
Cantilever anchorage
Cantilever anchorage with loading from a distant site to individual teeth or the archwire
Headgear
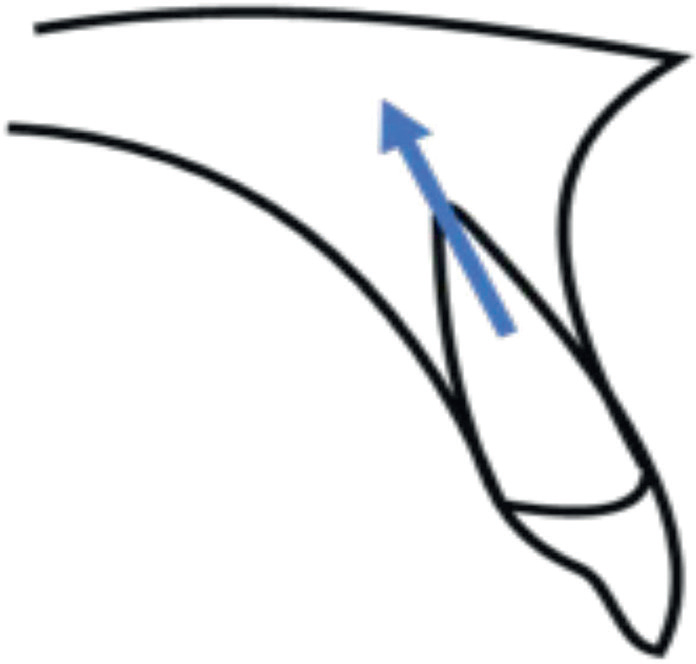
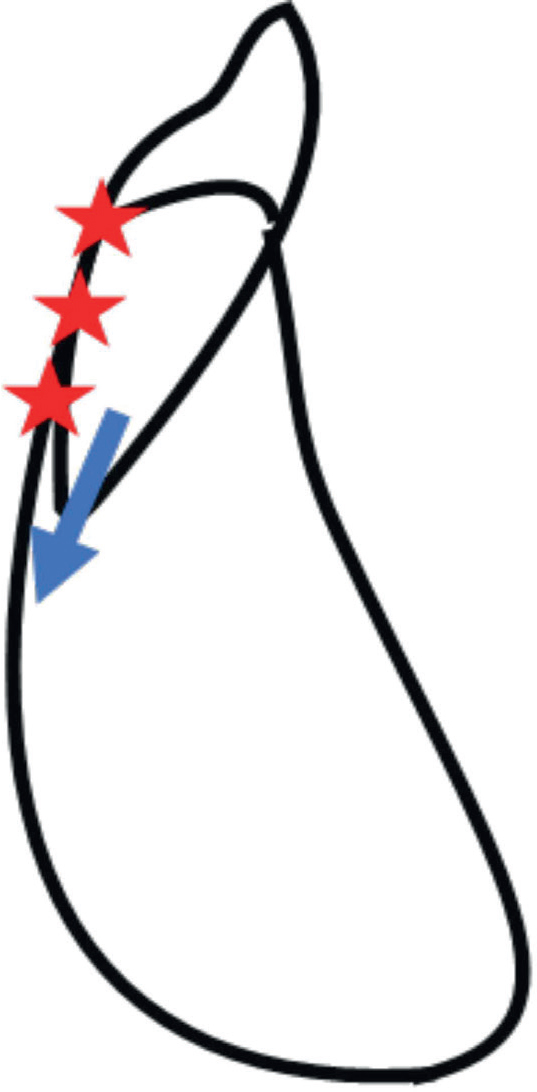
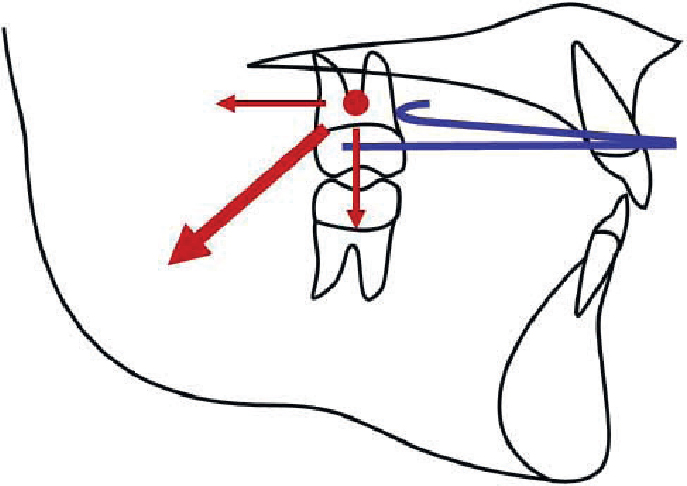
Cervical pull headgear in patients with increased anchorage demands can successfully reduce an increased overbite. The headgear applies force in a backwards and downwards direction (Figure 16), extruding the upper molar by directing the force through the centre of resistance of the tooth.11
Figure 16. Resultant force (depicted by large red arrow) when cervical headgear is used will not only distalize the upper molars, but lead to their extrusion into the back of the ‘wedge’, thereby reducing the overbite anteriorly.
Anteriorly placed high pull (J-hook) headgear to the upper archwire for intrusion of the upper labial segment teeth is no longer used owing to issues surrounding patient compliance, risk of root resorption and potential for eye injury.19
Aligners
A study has shown that aligners can reduce an overbite by 1.5 mm even though they cover the occlusal surfaces of all the teeth. This is principally the result of proclination of the mandibular incisors in combination with approximately 0.5 mm extrusion of the mandibular molars.20 However, one report highlighted the difficulties associated with overbite control using aligners, especially in cases with deep initial overbites, and suggested that over-engineering of the virtual set-up or use of auxiliary appliances may be necessary.21
Orthognathic surgery
If an adult patient presents with a severe Class 2 skeletal base with an increased overbite and reduced FMPA and ALFH, an orthognathic approach may be most appropriate. Typically, these patients have an increased COS and the pre-surgical orthodontics may include maintenance of the COS. This creates a ‘three-point landing’ at the time of surgery, with tooth contacts at the incisors and terminal molars bilaterally, which will help increase the ALFH. The resultant lateral open bites in the premolar regions are closed with extrusion mechanics as part of the post-surgical phase of treatment. Levelling the curve requires space, and this must be considered during treatment planning.7
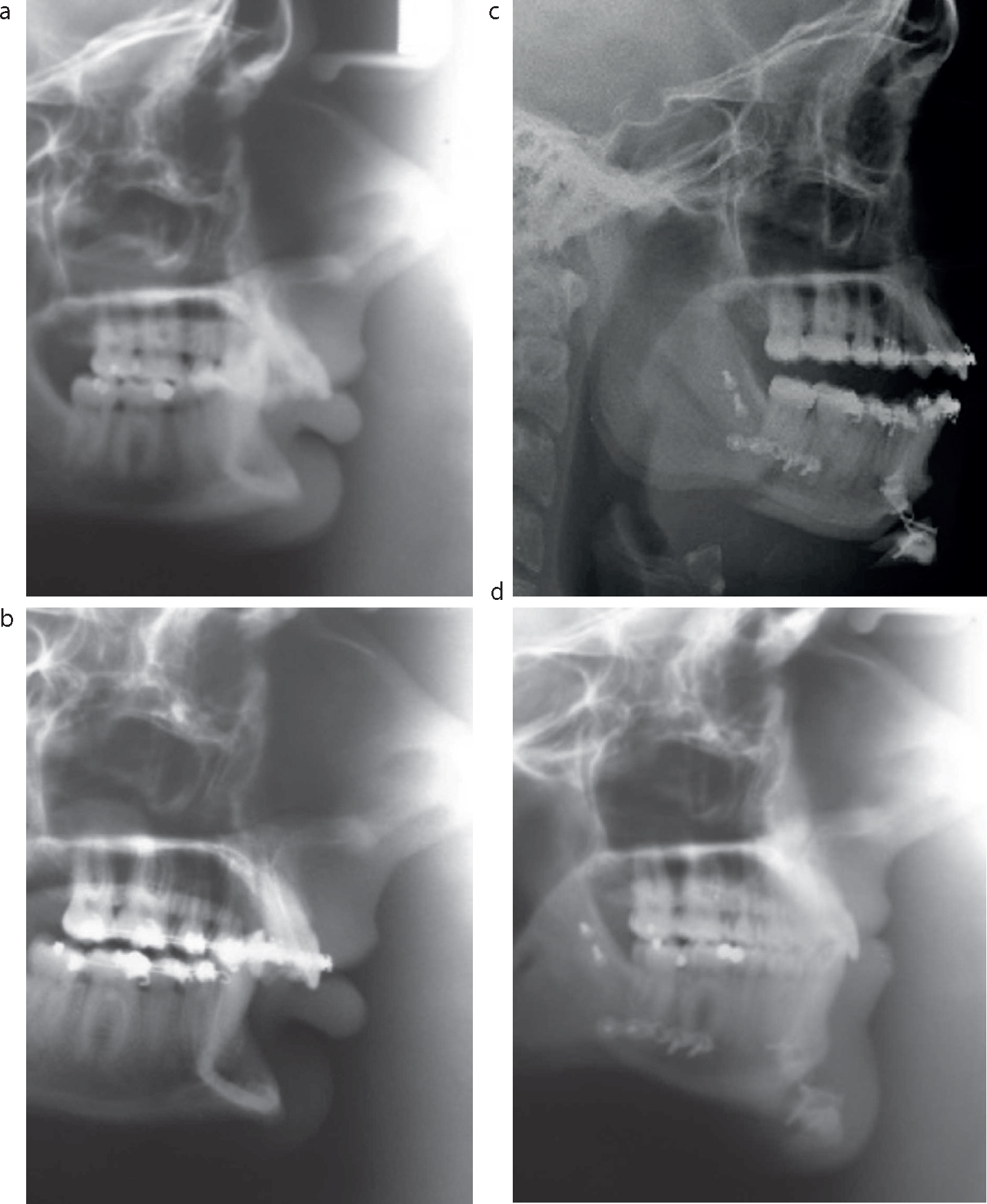
Other orthognathic approaches include the use of segmental osteotomies. These can be carried out in the maxilla and mandible to reduce the overbite. In addition, a downward sliding genioplasty and mandibulotomy can be carried out to increase the ALFH (Figure 17). In the pre-surgical orthodontic phase of treatment, the individual segments are aligned separately, with space created between the teeth at the sites of the surgical cuts.7
Figure 17. Bilateral sagittal split osteotomy advancement with downward sliding genioplasty. Post-advancement lower arch levelling was achieved with lower posterior extrusion. (a) Pre-treatment, (b) pre-surgical, (c) post-surgical, (d) end of treatment. Note the closure of the lateral open bite following the three-point landing (c) with the increased anterior lower face height retained (d).
Space closure in low angle cases
Anecdotally, patients presenting with a low angle are considered to demonstrate slower space closure than patients with an average or increased vertical dimension. However, a randomized controlled trial demonstrated that there was no such association between rate of space closure and FMPA, although there was a relationship between rate of space closure and gender, which was most likely to have been related to the timing of the pubertal growth spurt in the trial participants.22
No orthodontic treatment
It may not always be appropriate to treat an increased overbite with orthodontic treatment. Depending on the complaint and severity, alternative options may include a simple soft night guard or baseplate, or more complex restorative treatment. In the case of the latter, this may involve increasing the occlusal vertical dimension both posteriorly and anteriorly, ensuring anterior tooth-to-tooth contact to prevent overeruption of the incisors.23
Stability and retention
Relapse can be defined as the movement of teeth towards their initial positions.24 Overbite reduction is inherently unstable and the greater the pre-treatment overbite, the greater the tendency towards a deeper overbite long-term.25 Stability can be related to a number of factors, including:
Interincisal angle
Lower incisor tip to the upper incisor root centroid relationship
Unstable movements.
If an increased overbite is treated while the patient is still growing, the use of an anterior bite plane as part of the retention phase may be beneficial until facial growth has ceased.26
Conclusions
Diagnosis and treatment of patients with a low angle presents difficulties for the orthodontist. There are a variety of orthodontic methods available to reduce an increased overbite and the choice of appliance will depend on different factors. A holistic approach to managing these cases is recommended.