Baccetti T, Sigler LM, McNamara JA An RCT on treatment of palatally displaced canines with RME and/or a transpalatal arch. Eur J Orthod. 2011; 33:601-607 https://doi.org/10.1093/ejo/cjq139
Angell EC. Treatment of irregularities of the permanent or adult teeth. Dental Cosmos. 1860; 1:540-544
Inchingolo AD, Ferrara I, Viapiano F, Netti A, Campanelli M, Buongiorno S Rapid maxillary expansion on the adolescent patient: systematic review and case report. Children (Basel). 2022; 9 https://doi.org/10.3390/children9071046
Norton NS. Netter's head and neck anatomy for dentistry, 3rd edN. Philadelphia (PA): Elsevier, Health Sciences Division; 2021
Chaconas SJ, Caputo AA. Observation of orthopedic force distribution produced by maxillary orthodontic appliances. Am J Orthod. 1982; 82:492-501 https://doi.org/10.1016/0002-9416(82)90318-9
Sigler LM, Baccetti T, McNamara JA Effect of rapid maxillary expansion and transpalatal arch treatment associated with deciduous canine extraction on the eruption of palatally displaced canines: A 2-center prospective study. Am J Orthod Dentofacial Orthop. 2011; 139:E235-244 https://doi.org/10.1016/j.ajodo.2009.07.015
Vaughn GA, Mason B, Moon H-B, Turley PK. The effects of maxillary protraction therapy with or without rapid palatal expansion: A prospective, randomized clinical trial. Am J Orthod Dentofacial Orthop. 2005; 128:299-309 https://doi.org/10.1016/j.ajodo.2005.04.030
Almuzian M, Short L, Isherwood G, Al-Muzian L, Mcdonald J. Rapid maxillary expansion: a review of appliance designs, biomechanics and clinical aspects. Orthodontic Update. 2016; 9:90-95 https://doi.org/10.12968/ortu.2016.9.3.90
Schütz-Fransson U, Kurol J. Rapid maxillary expansion effects on nocturnal enuresis in children. Angle Orthod. 2008; 78:201-208 https://doi.org/10.2319/021407-71.1
Gray LP. Results of 310 cases of rapid maxillary expansion selected for medical reasons. J Laryngol Otol. 1975; 89:601-614 https://doi.org/10.1017/s0022215100080804
Bahammam SA. Rapid maxillary expansion for obstructive sleep apnea among children – systematic review and meta-analysis. Sleep Sci. 2020; 13:70-77 https://doi.org/10.5935/1984-0063.20190123
Bazargani F, Feldmann I, Bondemark L. Three-dimensional analysis of effects of rapid maxillary expansion on facial sutures and bones: a systematic review. The Angle Orthodontist. 2013; 83:1074-1082 https://doi.org/10.2319/020413-103.1
Krüsi M, Eliades T, Papageorgiou SN. Are there benefits from using bone-borne maxillary expansion instead of tooth-borne maxillary expansion? A systematic review with meta-analysis. Prog Orthod. 2019; 20 https://doi.org/10.1186/s40510-019-0261-5
Yacout YM, Abdalla EM, El Harouny NM. Skeletal and dentoalveolar effects of slow vs rapid activation protocols of miniscrew-supported maxillary expanders in adolescents: A randomized clinical trial. Angle Orthod. 2022; 92:579-588 https://doi.org/10.2319/112121-856.1
Liou EJ-W, Tsai W-C. A new protocol for maxillary protraction in cleft patients: repetitive weekly protocol of alternate rapid maxillary expansions and constrictions. Cleft Palate Craniofac J. 2005; 42:121-127 https://doi.org/10.1597/03-107.1
Suri L, Taneja P. Surgically assisted rapid palatal expansion: a literature review. Am J Orthod Dentofacial Orthop. 2008; 133:290-302 https://doi.org/10.1016/j.ajodo.2007.01.021
Needleman HL, Hoang CD, Allred E, Hertzberg J, Berde C. Reports of pain by children undergoing rapid palatal expansion. Pediatr Dent. 2000; 22:221-226
Greenbaum KR, Zachrisson BU. The effect of palatal expansion therapy on the periodontal supporting tissues. Am J Orthod. 1982; 81:12-21 https://doi.org/10.1016/0002-9416(82)90283-4
Barber AF, Sims MR. Rapid maxillary expansion and external root resorption in man: a scanning electron microscope study. Am J Orthod. 1981; 79:630-652 https://doi.org/10.1016/0002-9416(81)90356-0
Sandikçiolu M, Hazar S. Skeletal and dental changes after maxillary expansion in the mixed dentition. Am J Orthod Dentofacial Orthop. 1997; 111:321-327 https://doi.org/10.1016/s0889-5406(97)70191-4
Lanigan DT, Mintz SM. Complications of surgically assisted rapid palatal expansion: review of the literature and report of a case. J Oral Maxillofac Surg. 2002; 60(1):104-10 https://doi.org/10.1053/joms.2002.29087
Rapid maxillary expansion: a clinical insight for the general dental practitioner Jack Slaymaker Julian Woolley Sunil Hirani Dental Update 2024 16:4, 707-709.
Rapid maxillary expansion is an orthodontic treatment approach for corrections of transverse discrepancies, such as crossbites. Rapid maxillary expansion expands the palate by applying forces to the teeth and surrounding tissues to separate the mid-palatal suture, allowing for the correction of the indicated malocclusions. A general dental practitioner should be aware of the indications, treatment strategy and play an important role in the timely referral of patients for orthodontic assessment. This article offers a comprehensive overview of rapid maxillary expansion, expansion protocols, and an in-depth analysis of the prevalent characteristics associated with expansion, along with evidence-based recommendations for effective management.
CPD/Clinical relevance: This paper aims to give the general dental practitioner clinical insight into rapid maxillary expansion, the devices used and the indications for use.
Article
Rapid maxillary expansion (RME) is an orthodontic treatment used to expand the maxilla in the transverse plane. It can be used to correct posterior crossbites, relieve dental crowding and create space for impacted canines and in the correction of class III malocclusions.1,2.
RME involves using a specially designed appliance secured to the patient's maxillary teeth or palate. The appliance gradually widens the maxilla by exerting high forces on the bones that make up the palate. Over time, this force results in the separation of the mid-palatal suture leading to bony remodelling across the newly created space.
When seeing their regular patients, dentists may come across RME in either the active treatment or retention phases. For this reason, general dentists should have a clinical awareness of this procedure, particularly to communicate with patients and their relatives regarding the indications and observed effects of treatment. This article offers a comprehensive overview of RME, encompassing the history, anatomy, indication, various appliance options, expansion protocols and evidence-based recommendations for troubleshooting and management.
History of rapid maxillary expansion
The earliest cited report of RME is by E.C. Angell, published in Dental Cosmos in 1860. This involved a 14-year-old female patient with a transverse maxillary discrepancy. She was fitted with a device featuring two contrarotating screws, threaded left and right. The appliance relied on the pressure exerted on the necks of the molar teeth to stay in position instead of being cemented in place. As the screws were turned, heavy forces caused the arch to expand and correct the transverse discrepancy.3 The work was discredited at the time due to differing opinions about the palatal suture line and bony fusion rendering the viewpoint that Angell's observations were impossible and the results exceedingly doubtful.4
There were further attempts to reintroduce RME into the orthodontic catalogue in the early 20th century. However, it was Haas who repopularised the technique with his own design of an RME appliance in 1956, aptly called the ‘Haas expander’ which featured acrylic pads that rested in the lateral palatal walls.
Further developments by Biederman in 1968 led to the adoption of the popular and successful Hyrax expander. This was followed by Cohen and Silverman's equally popular bonded design in 1973. Currently, in a suitable patient, the expansion techniques of these designs are generally accepted as relatively simple, with predictable outcomes.5 As a result, RME is commonplace in the armamentarium of orthodontists.
Anatomy and physiology of the maxilla
The maxilla is a paired bone that forms the majority of the skeleton of the mid-face and upper jaw. The two bones are composed of five major parts:
The body
Frontal process
Zygomatic process
Palatine process
Alveolar process.
The latter four parts extend from the central pyramid-shaped body. The paired maxillary bones are joined via the intermaxillary (mid-palatal) suture line.6
Within the palatine process of the maxilla, the mid-palatal suture joins the two palatine bones at their horizontal plates and continues as an intermaxillary suture in the sagittal plane. The mid-palatal and the incisive suture form the junction of three opposing pairs of bones: the premaxilla, maxilla, and the palatine.7
The mid-palatal suture and its patency are crucial to the process of RME. During development, the absence of continuous fused bone over the suture site allows for the high forces of RME to separate the suture without surgery.
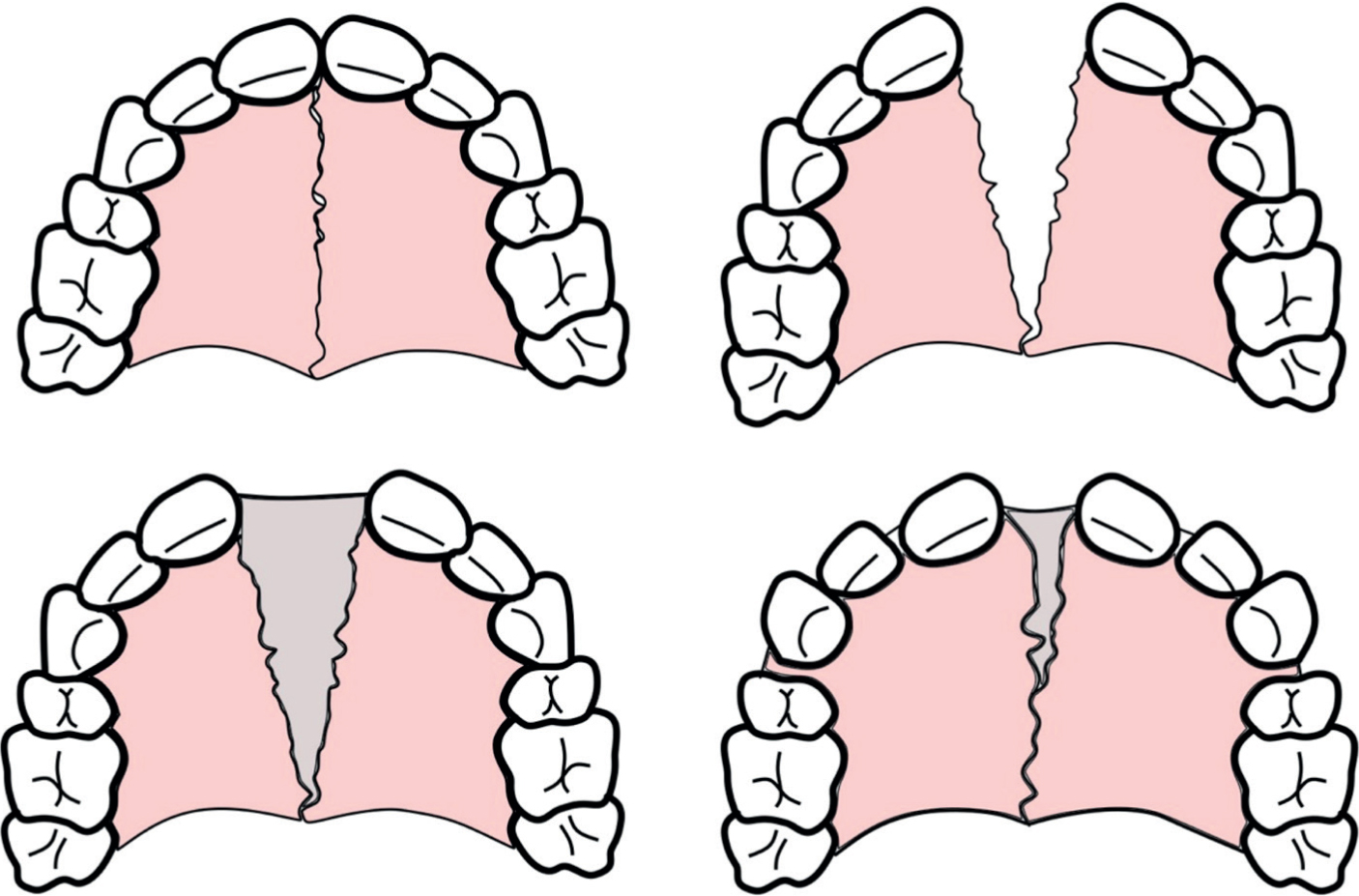
Once the appliance is activated, forces up to 4500g can be generated and exerted onto the left and right palatal shelves. Once orthopaedic separation of the shelves has occurred, further activations of the appliance result in continual separation at the mid-palatal suture. In this newly formed space, the tensional force generated results in osteoblastic differentiation and the production of new bone at the sutural edges. This process is also known as distraction osteogenesis (Figure 1).
Figure 1. Diagrammatic representation of the orthopaedic separation of the mid-palatal suture (top right), bony infill (bottom left) and subsequent reorganisation and remodelling (bottom right). Note the drifting of incisors into the incisal region following remodelling (bottom right).
The retention of the RME appliance is conducive to prevention of relapse. Keeping the device in place for a period of months allows for the reorganisation and remodelling process to complete in the maxillary suture in the newly formed position, therefore making it less prone to relapsing to the original position.8
According to the literature, the optimum age for RME is 10−14 years old, but this is gender dependent. Females present with increased interdigitation of the sutures earlier than their male counterparts, resulting in increased resistance to RME. This resistance and bone rigidity may limit the achievable expansion and the long-term stability of RME.9
As the human facial skeleton develops in late adolescence and early adulthood, the suture becomes increasingly interdigitated and as a result, the force required to initiate separation increases. In fact, complete ossification and fusion at the suture line may not occur until late adulthood. However, at this stage, RME becomes more difficult without surgical intervention.10,11 This is a result of the increased interdigitation of the palatine sutures and the increased rigidity of the maxillary bones producing a greater level of resistance to suture separation.12
RME is indicated in the following scenarios:
Patients with a posterior crossbite that is a result of a transverse discrepancy between the maxilla and mandible13
To relieve crowding. Expansion increases the arch width, meaning more space is generated in the arch, which can relieve crowding14
Interceptive treatment of impacted canines. Research has demonstrated an improvement in permanent canine positions with expansion and through space creation, there is more space for canines to erupt into the arch.15
Treatment of Class III malocclusions with concurrent use of additional treatments, such as protraction facemask therapy.16 The maxilla becomes increasingly interdigitated with the surrounding facial skeleton during adolescence. It is thought that expansion of the maxilla is able to disrupt the interdigitation and allow for protraction in patients with a class III skeletal base.
It is worth noting that RME has been suggested for other purposes, however these currently have insufficient literature to support their use:
Improve hearing in patients with conductive hearing loss.21
Types of rapid maxillary expansion appliances
The RME appliance design features an expansion screw incorporated into a framework which is supported by either the teeth (tooth-borne), teeth and soft tissues (tooth-tissue borne), teeth and the bone (tooth-bone borne) or solely the bone (bone borne).
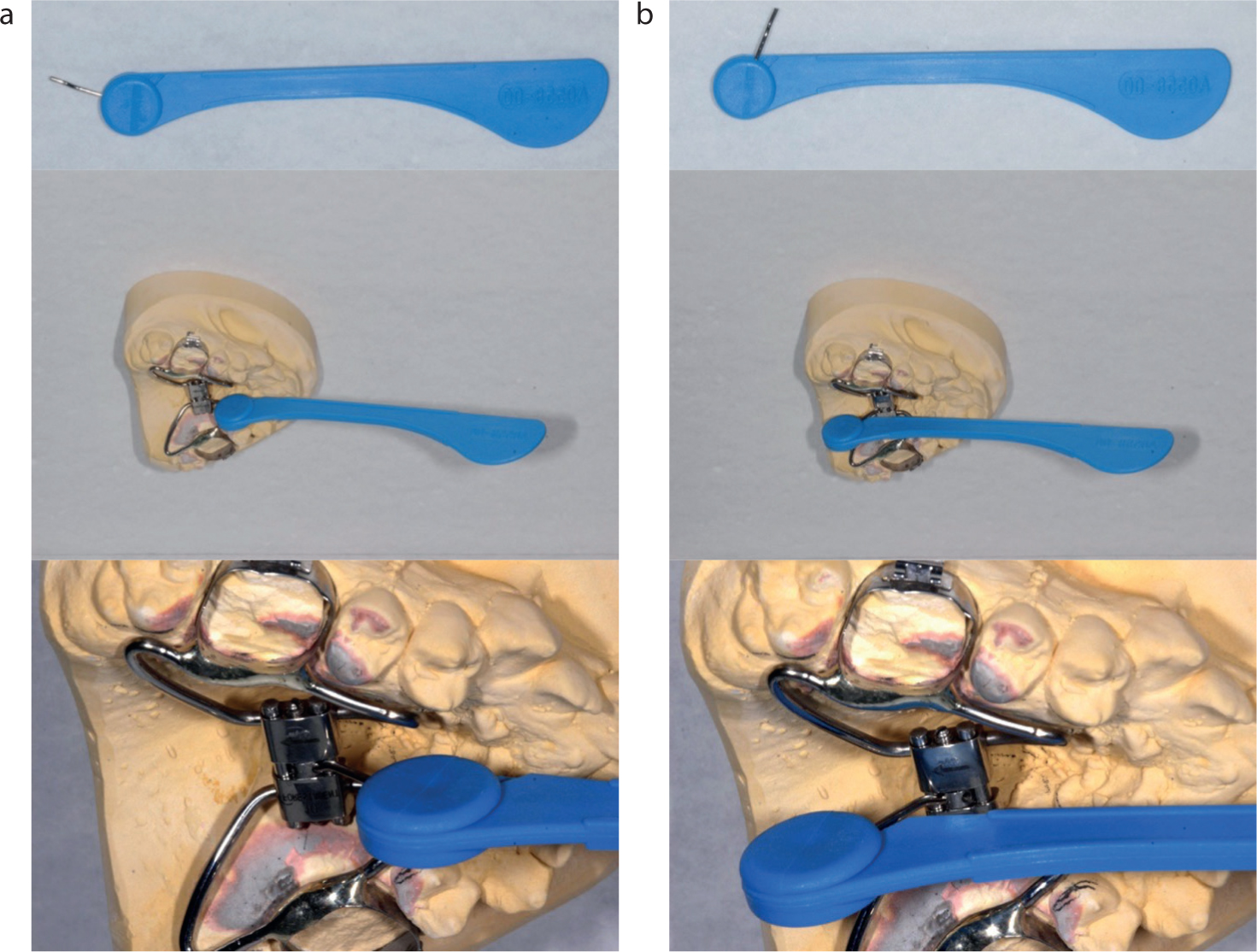
The size of the expansion screw can vary depending on the patient's clinical needs but typically range from 8–12mm, and activation is achieved using a turning key (Figure 2). A parent or carer will be required to place the key, with the correct orientation, into the keyhole in the centre of the expansion screw and then gently push the key towards the back of the mouth (Figure 3).
Figure 2. A rapid maxillary expansion screw. An arrow may be printed on the screw to aid the operator in the correct direction of activation. The keyhole is visible in the middle of the screw.Figure 3. Insertion (a) and activation (b). The orientation of the turning key (top left) with the humps facing away from the maxillary teeth allows for correct activation. The design of the rapid maxillary expansion turning key allows for easier activation in the posterior oral cavity.
The screw and key are self-limiting and will stop after one turn. One turn is equivalent to ¼ of the full rotation of the screw, resulting in 0.2–0.25mm of expansion depending on the screw type. Issues may arise if the screw is not fully turned, as the parent or carer will have difficulty locating the keyhole on the subsequent activation (Figure 3).
One turn or ‘activation’ is equivalent to 0.25mm expansion at the screw. However, expansion of the screw is not a 1:1 ratio to the expansion at the mid-palatal suture and will vary depending on RME design.22 Compared to other methods of orthodontic expansion, RME devices operate with a much higher force to produce the desirable orthopaedic effects.8
Tooth-borne and tooth-tissue borne
The Hyrax appliance (tooth-borne) and the Haas appliance (tooth-tissue borne) are two popular designs for RME devices, and subtle modifications may be made for specific treatment objectives. The framework can be attached to the supporting teeth using stainless steel bands or occlusal capping made from cobalt chrome or acrylic.
The Hyrax appliance features an expansion screw directly soldered to bands cemented on the supporting teeth or incorporated into acrylic cemented to the teeth. The Hyrax design is more conducive to maintaining an optimal oral hygiene level than alternative configurations (Figure 4 and 5). The bonded design offers advantages in opening the bite to allow unhindered expansion.
Figure 4. A Hyrax-type appliance with bands fitted on the maxillary first molars and first premolars.Figure 5. A bonded-style Hyrax-type appliance bonded to the posterior teeth with acrylic capping. A variation in the design has been made with a ‘palatal split’ screw and metal arms for ease of removal.
The Haas-style appliance features an expansion screw attached to a palatal framework made of either acrylic or metal. This framework is soldered or welded to either bands or integrated into a capping element for bonded appliances. It is hypothesised that the tissue-borne palatal element enables the device to deliver more uniform expansion forces to the alveolar components. The disadvantage of this design is the potential iatrogenic irritation to the palatal tissue.
Evidence suggests that these appliances expand the mid-palatal suture at a percentage of 20–50% of the total screw length.22
Bone-borne and tooth-bone borne
Bone-borne devices, known as ‘mini-screw-assisted rapid palatal expanders’ (MARPE), are supported using temporary anchorage devices (TADs) (Figure 6). TADs, or mini-screws, are constructed from titanium alloys and are used to provide stable anchorage for orthodontic treatment. Unlike dental implants, TADs do not osseointegrate and can be easily removed following orthodontic treatment. Tooth-bone-borne devices, known as hybrid-RME appliances, gain support from both the teeth and TADs in the palatal bone (Figure 7).
Figure 6. A bone-borne mini-screw-assisted rapid palatal expander appliance. The temporary anchorage devices are placed, a ‘pick-up’ impression is taken and the appliance is fabricated. The appliance is then fitted and screwed into the temporary anchorage devices.Figure 7. A direct mini-screw-assisted rapid palatal expander appliance. The rapid maxillary expansion appliance is first cemented (a) and temporary anchorage devices placed afterwards through the corresponding insertion holes (b).
The advent of CAD-CAM technology has resulted in a plethora of designs for these appliances. Broadly, they can be categorised into indirect or direct appliances.
Indirect appliances involve the placement of TADs followed by a pick-up impression or digital scan. This is used to manufacture the appliance, which includes corresponding copings to seat over the TADs. The appliance is then seated onto the TADs and secured with connecting screws (Figure 6).
Direct appliances do not involve a pick-up impression and instead are first seated into the correct position, and TADs are inserted directly through corresponding holes in the appliance. This method reduces inaccuracies with impressions, scanning and laboratory stages (Figure 7).
The advantage of MARPE or hybrid-RME devices is the reduction in the deleterious dental effects caused by tooth-borne appliances, such as dental tipping and periodontal damage on the anchor teeth, such as fenestrations and dehiscence. In addition, these devices have been shown to present advantages in terms of increased sutural opening, resulting from the increased forces directed to the mid-palatal suture.23
Protocol for treatment
Following the appliance's fit, the parent, patient or carer will be instructed to activate the device following a specific regime. Regimes of activation will differ depending on the orthodontist, but will range from 1–2 activations per day for approximately 3 weeks with conventional tooth-borne RME devices. Studies estimate the approximate change in the intercanine width is 4mm, with greater sutural opening using bone-borne devices.23 Activations should be at regular intervals to allow the dissipation of forces and prevent compounded loads.8
Owing to the larger forces directed through the mid-palatal suture with bone-borne RME devices, slower activation regimes have been suggested to prevent excessive stress and TAD failure. Recent evidence on hybrid-RME appliances demonstrated that a regime of one activation every 2 days resulted in less untoward dental effects and TAD failures.24
Another infrequent and aptly named activation regime is alternate rapid maxillary expansion and contraction (alt-RAMEC). This protocol alternately expands and contracts the maxilla over 9 weeks to stimulate growth at the circum-maxillary sutures. Alt-RAMEC is typically carried out in patients with a class III skeletal base to enhance the effectiveness of maxillary protraction treatment.25
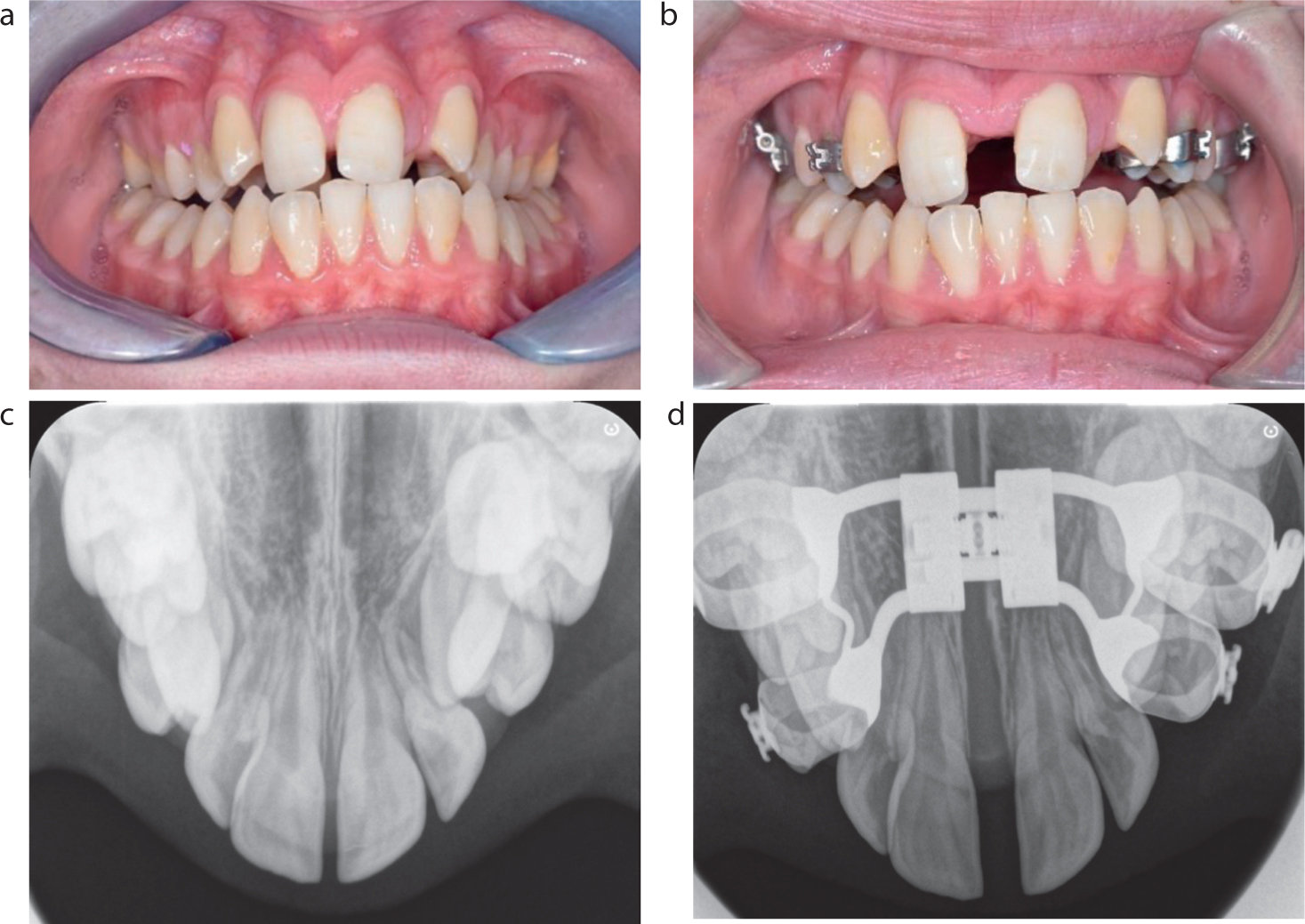
It is common for the orthodontist to review the patient during the active expansion period. The typical sign of mid-palatal suture patency is the appearance of a midline diastema (Figure 8). This is confirmed radiographically with an upper-standard occlusal radiograph (Figure 8). The orthodontist will also measure the extent of dental expansion and assess for complications. Patients should be made aware that the midline diastema is temporary and will spontaneously reduce after the expansion's completion.
Figure 8. (a–d) Pre- and post-rapid maxillary expansion over 3 weeks. Note the appearance of a midline diastema, correction of bilateral crossbite and the visible patency of the mid-palatal suture in the upper standard occlusal radiograph.
The expansion will often be concluded when the palatal cusps of the maxillary molar teeth align with the buccal cusps of the mandibular molar teeth. The overexpansion of the maxilla is carried out to compensate for an expected amount of relapse.
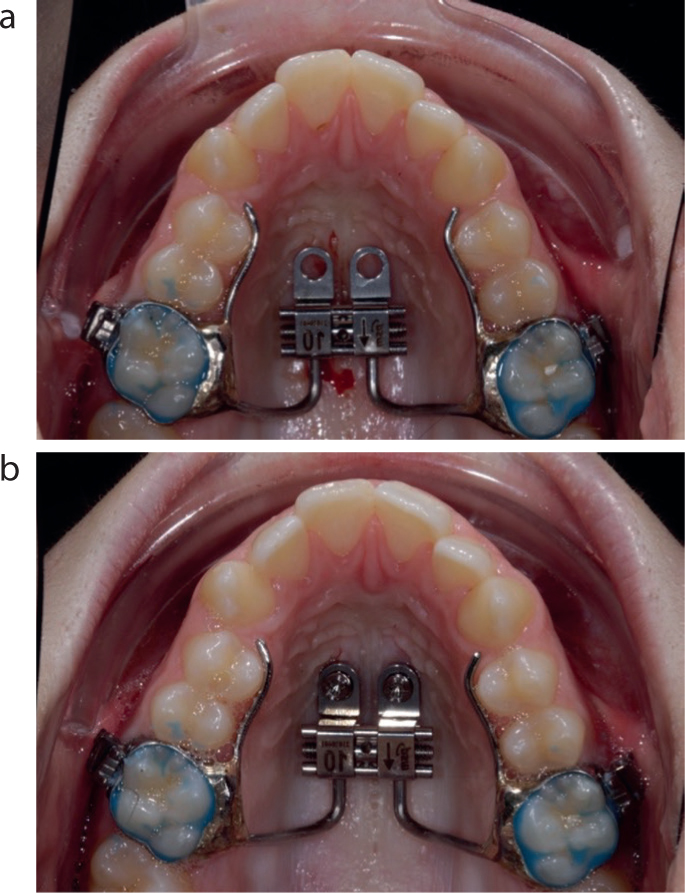
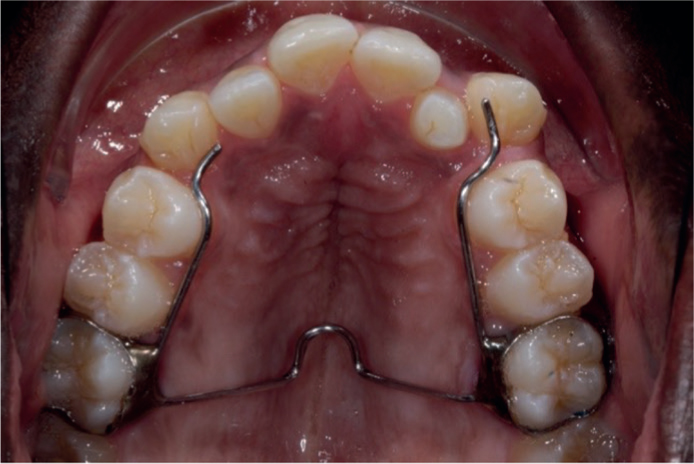
Different regimes exist following the completion of the expansion and these will depend on the need for further orthodontic treatment. The appliance will often be left in place for a minimum of 3 months to allow for bony infill of the mid-palatal suture and to prevent relapse of the expansion. To prevent continual activation, composite may be placed into the activation screw. After this period, if further treatment is required, it is not uncommon to retain the appliance in-situ, particularly if TADs will be required for other orthodontic treatment mechanics. However, the RME can also be substituted for a more comfortable trans-palatal arch (Figure 9). Once treatment has been completed, a Hawley-type retainer is suggested. A Hawley retainer has palatal coverage and therefore is more suitable to maintain the transverse expansion rather than typical vacuum-formed retainers.17
Figure 9. Following expansion and a retention period, the rapid maxillary expansion appliance can be removed and a trans-palatal arch with arms can be fitted
Surgically-assisted rapid palatal expansion
As mentioned previously, the increased interdigitation of the mid-palatal suture, particularly in older patients may impact the success of RME. Surgically-assisted rapid palatal expansion (SARPE) is an alternative treatment for skeletally mature individuals and involves a surgical split along the mid-palatal suture followed by a period of RME. To prevent damage to the central incisors during surgery, pre-surgical orthodontics can create a midline diastema and diverge the roots of the central incisors. Significant expansion can be achieved with SARPE, and in general, most reports state that surgical expansion is more stable than conventional RME.26
Clinical considerations and complications to be aware of
The most common side effect of RME is pain and discomfort experienced by the patient during the active phase of treatment. However, there are several other clinical considerations and possible complications. The degree of interdigitation is a limiting factor in prescribing RME and tooth-borne RME is typically less successful in patients above the age of 14. The advent of bone-anchored RME has allowed for much larger forces to separate the suture, thus the upper age limit for this treatment is higher.
As with all interventions, achieving consent for this procedure requires a discussion of the risks and potential complications with both patients and their parents. These include:
Pain and discomfort during activations
Failure to separate the mid-palatal suture
Debonding of appliance
Excessive tipping of posterior teeth
Formation of anterior open bites
Periodontal effects include recession, dehiscence or fenestrations
Development of temporary midline diastema during treatment
Gingival inflammation and irritation around the appliance
Gingival overgrowth around appliances (more common in MARPE or hybrid-RME)
Decalcification or caries around bands or occlusal capping
Speech difficulties
Relapse of expansion
Rarer complications include nosebleeds and dizziness on activations.27,28,29,30,31
Conclusions
Rapid maxillary expansion is considered a routine and effective orthodontic treatment for multiple malocclusions.
There are a number of RME designs available to orthodontists, each with similar protocols, advantages and disadvantages. The Hyrax (banded) appliance is one of the most popular RME appliances and is likely to be frequently encountered by general dentists. Dentists must stay clinically aware of common treatments in orthodontics and be able to discuss the common side-effects of said treatments.
The success of orthopaedic separation is dependent on a number of factors, chiefly the level of interdigitation at the suture. The effectiveness of treatment is dependent on treatment during this window of development, beyond which the treatment becomes less predictable. Therefore, it is imperative to identify malocclusions early and consider timely referrals and interventions.