Bekri S, Trifi W, Labidi A, Bizani C, Mansour L Full-mouth rehabilitation of an acromegaly disease patient with removable prostheses: A clinical case report. Pan Afr Med J. 2019; 33:1-9 https://doi.org/10.11604/pamj.2019.33.5.18194
Sharma G, Amin D, Shorafa M Challenges in the management of late developing malocclusions in adulthood: A case report of acromegaly. J Orthod. 2019; 46:349-357 https://doi.org/10.1177/1465312519869943
Nakano H, Mishima K, Matsushita A Orthognathic surgery in an acromegalic patient with obstructive sleep apnea syndrome. Sleep Breath. 2013; 17:29-32 https://doi.org/10.1007/s11325-012-0711-5
Tuncer B, Bavbek N, Ozkan C Craniofacial and pharyngeal airway morphology in patients with acromegaly. Acta Odontol Scand. 2015; 73:433-440 https://doi.org/10.3109/00016357.2014.979868
Cassoni A, Pucci R, Priore P, Fadda MT, Valentini V Surgical management of the acromegalic face: Could the aesthetic improvement of the face influence the patient's QoL? Combined surgical approach. Oral Maxillofac Surg Cases. 2020; 6 https://doi.org/10.1016/j.omsc.2020.100150
Kernen FR, Bidra AS Dental Implant Therapy in a Patient with Acromegaly: A Clinical Report. J Prosthodont. 2019; 28:355-360 https://doi.org/10.1111/jopr.13043
Din A, Bhatti N A multidisciplinary approach to management of facial deformity in Acromegaly: a case report. Br J Oral Maxillofac Surg. 2014; 52:e117-e118 https://doi.org/10.1016/j.bjoms.2014.07.226
Tuthill A, McKenna T, O'Shea D Iatrogenic Acromegaly. Endocr Abstr. 2002; 3
The development of malocclusion in adulthood presents diagnostic and management challenges. The aetiology of any changes must be identified because this will influence patient management, particularly if surgical intervention is considered.
CPD/Clinical Relevance: This case demonstrates the importance of both awareness and clinical suspicion of acromegaly and highlights a novel aetiology of the disease.
Article
Acromegaly is an acquired adult endocrine disorder caused by excessive levels of growth hormone and insulin-like growth factor (IGF-1). In adults, excess growth hormone and IGF-1 result in abnormal growth, including characteristic craniofacial and dental changes, often caused by a pituitary adenoma or concomitant endocrinological involvement.1,2 Chronic exposure to excessive levels of growth hormone and IGF-1 is associated with significant morbidity and mortality.1,3
In this report, a review of the literature along with a case of acromegaly is presented, with atypical aetiology where exogenous growth hormone replacement therapy was prescribed as treatment for panhypopituitarism following pituitary tumour removal.
Effect of increased growth hormone in adults
High levels of growth hormone stimulate cell proliferation and differentiation of both hard and soft tissues, causing enlargement of the hands, feet, forehead, jaw and nose. These physical changes result in broad hands and feet, thickened skin, with patients typically complaining of ring or shoe-size changes. Other changes include soft tissue swelling, increased nasal prominence, thick nails, large pores, deepening nasolabial and forehead creases and oedematous eyelids.4
Acromegaly can lead to systemic complications such as glucose intolerance, headaches, cardiovascular problems, joint problems, respiratory conditions such as sleep apnoea, lipid metabolism disorders, goitre, skin tags and myalgia.3,5
Dental features
A recent study found that 81% of acromegaly patients were affected by oral or dental problems.2
A Class III malocclusion is the most typical feature, with a reported frequency between 25% and 77%, with average overjet of −9 mm.3,6 It is often bilateral and symmetrical,6,7 but can be asymmetrical.3,4
Patients typically complain of a change in occlusion or difficulty eating, alongside other orofacial changes,1 including macroglossia, anterior open bite, lip incompetence, mandibular diastema, mandibular tooth mobility, thickened gingivae, and thickened lips.4,6,8
Diagnosis of acromegaly
Presenting facial, oral and dental problems may lead to an initial diagnosis of acromegaly. A recent study found the most frequent symptoms were tooth related,2 meaning dentists and orthodontists are uniquely poised to identify underlying disorders, which may otherwise go unnoticed, and be the first healthcare provider to diagnose the patient.6
It is reported that although 41% of patients presented to a dental professional, acromegaly was only suspected in 5% of cases.2 It is therefore essential that awareness of the disease is raised among all healthcare professionals who may consult undiagnosed patients. A timely diagnosis may limit potential facial disfigurement, reduce the treatment burden and improve patients' quality of life.3
Radiographs
An orthopantomogram and lateral cephalogram are often useful in diagnosis. An orthopantomogram may reveal elongated condyles and coronoid process, root hypercementosis and increased alveolar density. A lateral cephalogram may show expansion of the frontal sinuses and an enlarged sella turcica, reduced pharyngeal airway dimensions, steep mandibular plane with increased vertical proportions and a skeletal Class III profile.1,4,6
Treatment of acromegaly
Biochemical screening will confirm that serum levels of growth hormone and IGF-1 are raised; however, the underlying cause must still be determined. If a pituitary tumour is suspected, an MRI is the gold standard imaging modality, although plain films can show sella turcica enlargement in some cases. Treatment depends on the underlying cause, but can include surgery, radiation and pharmacological treatment.4 In this case, exogenously prescribed growth hormone replacement therapy was the underlying cause and supplementation was simply stopped.
Treatment of the residual deformity
Once disease control is assured, and the patient medically stable, multidisciplinary treatment should be undertaken. A thorough evaluation of fitness for surgical treatment, and monitoring thereafter, will be required.4,8
Treatment planning
The aims of treatment are to restore function and aesthetics to their predisease state, therefore, a combined approach is required, integrated between orthodontists, orthognathic surgeons and prosthodontists.3 Close liaison will be required with endocrinologists, the general medical practitioner and practitioners of any other relevant specialties.4,7,8
The extent of the deformity should be defined and clear treatment aims determined, which may include: correction of skeletal deformity, correction of malocclusion, improvement of airway proportions, improvement of the soft tissue profile and prosthetic rehabilitation.3,7
Treatment of patients has included combined orthodontic and orthognathic surgery (often bimaxillary)4,5,7,9 glossectomy,5,7 adjunctive plastic surgery (rhinoplasty)7 and prosthetic rehabilitation, including implant placement.3,8,9
Case report
This case report highlights a rare aetiology of acromegaly and demonstrates the important role of the dental profession in initial diagnosis of the condition.
A 42-year-old male was referred by his general dental practitioner to the orthodontic department at Glasgow Dental Hospital, complaining of facial and occlusal changes. He noted that his front teeth no longer met and felt he had developed a lisp and deepening of his voice. His hands and feet were enlarging, and his nose was constantly blocked.
Extra-oral assessment
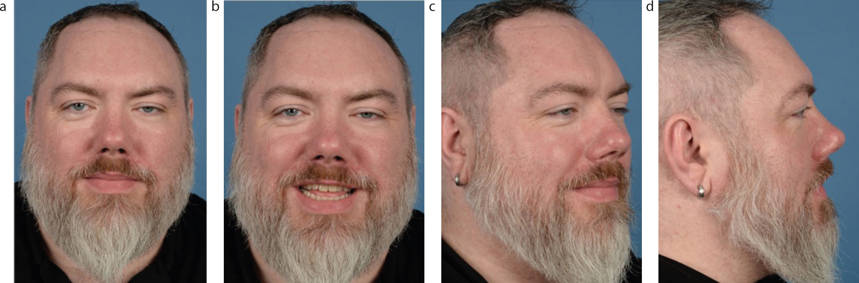
On examination, despite presenting with facial hair, a Class III skeletal base was noted with increased lower anterior facial height (Figure 1). The chin point deviated slightly to the left-hand side; the lips were competent, and incisal show was average at rest and on smiling.
Figure 1. (a–d) Extra-oral clinical photographs.
Intra-oral assessment
All permanent teeth were present and erupted. In occlusion, the incisal relationship was Class III, with a negative overjet of 2 mm and anterior open bite of 5 mm, extending to the premolars. The molar relationship was a half-unit Class III bilaterally, as were the canines. There were bilateral crossbites extending from the first premolar to the second molar, with no associated displacement. The upper dental midline was coincident with the mid-sagittal plane; the lower dental midline was deviated to the left by approximately 1 mm. The upper and lower arches were well aligned, with a mildly proclined lower labial segment. Oral hygiene was fair with marginal gingivitis localized to the anterior segment; the oral mucosa was healthy (Figure 2).
Figure 2. (a–e) Intra-oral clinical photographs.
Radiographic assessment
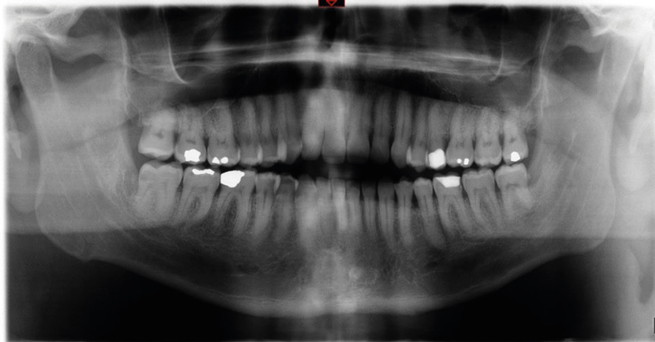
An orthopantomogram (Figure 3) displayed moderately restored dentition, with caries affecting the lower right second and third molars and the lower left first molar. Mild horizontal bone loss was noted in the lower left premolar region. There was suggestion of hypercementosis affecting the lower left second premolar, and of increased alveolar density in the symphyseal region. The condylar heads appeared elongated and pulpal stones were noted throughout the dentition. The lateral cephalogram (Figure 4) confirmed a mild Class III skeletal pattern with increased lower anterior facial height. The upper incisors were of average inclination and the lowers were slightly proclined. The sella turcica had reduced morphological dimensions.
A diagnosis of acromegaly was suspected, and a thorough medical history obtained.
The patient was diagnosed with craniopharyngioma in August 2015, after suffering visual disturbances and headache; an MRI demonstrated a suprasellar mass compressing the optic nerve. He underwent a right pterional craniotomy and sub-total excision of the space-occupying lesion. The pathological diagnosis was consistent with craniopharyngioma and post-operative radiotherapy was advocated, which was completed in November 2015.
Following treatment, the patient experienced improvement in vision but was left with panhypopituitarism as a result of his surgery. He was referred to an endocrinology department for ongoing care, including a hormone replacement regimen.
In June 2017, he was diagnosed with growth hormone deficiency by an endocrinologist and started growth hormone replacement therapy in September 2017. In December, his growth hormone levels were found to be adequate. In April 2018, his dose was reduced because of an elevated IGF-1 serum level of 259 µg/L (reference range 63–201 µg/L). It was reduced again in October as his IGF-1 levels remained elevated at 272 µg/L; which is when symptoms of acromegaly were noted, and he was referred to to the dental hospital. At this point, he had been taking growth hormone for 13 months.
Management
A letter was sent to the patient's endocrinologist regarding the suspicion of acromegaly and on their recommendation, growth hormone replacement ceased in February 2019, after a total 17-month supplementation. In April 2019, he was formally diagnosed with iatrogenic acromegaly through exogenous administration of excess growth hormone.
By May 2019, his IGF-1 levels were found to be within the normal range at 113ug/L, and there are no plans to restart growth hormone replacement.
Treatment
On review in February 2020, the patient had no progression of symptoms. A lateral cephalogram was exposed showing small changes, with a slight improvement in ANB angle and lower incisor inclination. The patient was scheduled for a joint orthodontic/orthognathic clinic, however, due to the pandemic, it was some time before further management could be undertaken.
There has been only one other case of iatrogenic acromegaly reported in the literature, emphasising the vigilance required by the dental profession. An eye for pattern recognition and a holistic assessment of the patient considering their medical history and current complaints is essential.10
Summary
A review of the current literature is presented along with a case report highlighting an unusual aetiology for acromegaly. It demonstrates that the dental professional is often the first healthcare professional seen by patients with this condition. With irreversible and debilitating facial and occlusal changes, iatrogenic acromegaly represents a condition the dental profession is uniquely poised to initially diagnose, potentially limiting the negative sequelae.