Samsonyanová L, Broukal Z. A systematic review of individual motivational factors in orthodontic treatment: facial attractiveness as the main motivational factor in orthodontic treatment. Int J Dent. 2014; https://doi.org/10.1155/2014/938274
Gustafsson M, Ahlgren J. Mentalis and orbicularis oris activity in children with incompetent lips: An electromyographic and cephalometric study. Acta Odontol Scand. 1975; 33:355-363 https://doi.org/10.3109/00016357509004640
Harradine N, Kirschen R. Lip and mentalis activity and its influence on incisor position—a quantitative electromyographic study. Br J Orthod. 1983; 10:114-127 https://doi.org/10.1179/bjo.10.3.114
Negruţiu B, Vaida L, Todor B, Judea A, Lile I, Moca A, Judea-Pusta C. An important morphological feature of the face: upper lip length. Rom J Morphol Embryol. 2019; 60:537-541
Pecora N, Baccetti T, McNamara J. The aging craniofacial complex: a longitudinal cephalometric study from late adolescence to late adulthood. Am J Orthod Dentofacial Orthop. 2008; 134:496-505 https://doi.org/10.1016/j.ajodo.2006.11.022
Lambrechts H, De Baets E, Fieuws S, Willems G. Lip and tongue pressure in orthodontic patients. Eur J Orthod. 2010; 32::466-471 https://doi.org/10.1093/ejo/cjp137
Wong W, Davis D, Camp M, Gupta S. Contribution of lip proportions to facial aesthetics in different ethnicities: a three-dimensional analysis. J Plast Reconstr Aesthet Surg. 2010; 63:2032-2039 https://doi.org/10.1016/j.bjps.2009.12.015
Houlton T, Jooste N, Steyn M, Hemingway J. Visualising trends in dentition to lip mouth morphology using geometric morphometrics. PLoS One. 2022; 17 https://doi.org/10.1371%2Fjournal.pone.0274127
Wollina U. Perioral rejuvenation: restoration of attractiveness in aging females by minimally invasive procedures. Clin Interv Aging. 2013; 8:1149-1155 https://doi.org/10.2147/cia.s48102
Wen Y, Wong H, Lin R, Yin G, McGrath C. Inter-Ethnic/Racial Facial Variations: A Systematic Review and Bayesian Meta-Analysis of Photogrammetric Studies. PLoS One. 2015; 10 https://doi.org/10.1371/journal.pone.0134525
Drobocky O, Smith R. Changes in facial profile during orthodontic treatment with extraction of four first premolars. Am J Orthod Dentofacial Orthop. 1989; 95:220-230 https://doi.org/10.1016/0889-5406(89)90052-8
Konstantonis D, Vasileiou D, Papageorgiou S, Eliades T. Soft tissue changes following extraction vs. nonextraction orthodontic fixed appliance treatment: a systematic review and meta-analysis. Eur J Oral Sci. 2018; 126:167-179 https://doi.org/10.1111/eos.12409
Naini F, Cobourne MT, Garagiola U, McDonald F, Wertheim D. Mentolabial angle and aesthetics: a quantitative investigation of idealized and normative values. Maxillofac Plast Reconstr Surg. 2017; 39 https://doi.org/10.1186/s40902-017-0102-8
Pedretti C. Leonardo da Vinci: Notebook of a Genius.Milan (IT): Powerhouse Publishing; 2001
Duchenne G. The mechanism of human facial expression or an electro-physiological analysis of the expression of the emotions.New York (US): Cambridge University Press; 1990
Desai S, Upadhyay M, Nanda R. Dynamic smile analysis: changes with age. Am J Orthod Dentofacial Orthop. 2009; 136:310.E1-310.E10 https://doi.org/10.1016/j.ajodo.2009.01.021
Arnett G, Bergman R. Facial keys to orthodontic diagnosis and treatment planning – Part II. Am J Orthod Dentofacial Orthop. 1993; 103:395-411 https://doi.org/10.1016/s0889-5406(05)81791-3
Robbins J. Differential diagnosis and treatment of excess gingival display. Pract Periodont Aesthet Dent. 1999; 11:265-272
Springer N, Chang C, Fields H, Beck F, Firestone A, Rosenstiel S, Christensen J. Smile esthetics from the layperson's perspective. Am J Orthod Dentofacial Orthop. 2011; 139:E91-E101 https://doi.org/10.1016/j.ajodo.2010.06.019
Ker A, Chan R, Fields H, Beck M, Rosenstiel S. Esthetics and smile characteristics from the layperson's perspective: a computer-based survey study. J Am Dent Assoc. 2008; 139:1318-1327 https://doi.org/10.14219/jada.archive.2008.0043
Ugolini A, Agostino P, Silvestrini-Biavati A, Harrison J, Batista K. Orthodontic treatment for posterior crossbites. Cochrane Database Syst Rev. 2021; 12 https://doi.org/10.1002/14651858.cd000979.pub3
Holdaway R. A soft-tissue cephalometric analysis and its use in orthodontic treatment planning. Part II. Am J Orthod. 1984; 85:279-293 https://doi.org/10.1016/0002-9416(84)90185-4
Hajeer M, Ayoub A, Millett D, Bock M, Siebert J. Three-dimensional imaging in orthognathic surgery: the clinical application of a new method. Int J Adult Orthodon Orthognath Surg. 2002; 17:318-330
Ismail S, Moss J, Hennessy R. Three-dimensional assessment of the effects of extraction and nonextraction orthodontic treatment on the face. Am J Orthod Dentofacial Orthop. 2002; 121:244-256 https://doi.org/10.1067/mod.2002.121010
Janson G, Mendes L, Junqueira C, Garib D. Soft-tissue changes in Class II malocclusion patients treated with extractions: a systematic review. Eur J Orthod. 2016; 38:631-637 https://doi.org/10.1093/ejo/cjv083
Talass M, Talass L, Baker R. Soft-tissue profile changes resulting from retraction of maxillary incisors. Am J Orthod Dentofacial Orthop. 1987; 91:385-394 https://doi.org/10.1016/0889-5406(87)90391-x
Mandrekar P, Dhupar V, Akkara F. Prediction of Soft-Tissue Changes Following Single and Bi-Jaw Surgery: An Evaluative Study. Ann Maxillofac Surg. 2021; 11:32-36 https://doi.org/10.4103/ams.ams_138_20
Suh H, Lee H, Lee Y, Eo S, Donatelli R, Lee S. Predicting soft tissue changes after orthognathic surgery: The sparse partial least squares method. Angle Orthod. 2019; 89:910-916 https://doi.org/10.2319%2F120518-851.1
Nagori H, Fattahi T. Maxillary advancement surgery and nasolabial soft tissue changes. IOSR J Dent Med Sci.. 2017; 16:23-29 https://doi.org/10.9790/0853-1603082329
Rosenberg A, Muradin M, van der Bilt A. Nasolabial esthetics after Le Fort I osteotomy and V-Y closure: a statistical evaluation. Int J Adult Orthodon Orthongnath Surg. 2002; 17:29-39
Mahsoub R, Naini F, Patel S, Wertheim D, Witherow H. Nasolabial angle and nasal tip elevation changes in profile view following a Le Fort I osteotomy with or without the use of an alar base cinch suture: a long-term cohort study. Oral Surg Oral Med Oral Pathol Oral Radiol. 2020; 130:379-386 https://doi.org/10.1016/j.oooo.2020.05.011
Olivetti E, Nicotera S, Marcolin F, Vezzetti E, Sotong J, Zavattero E, Ramieri G. 3D Soft-Tissue Prediction Methodologies for Orthognathic Surgery—A Literature Review. Appl Sci. 2019; 9 https://doi.org/10.3390/app9214550
Lin S, Kerr W. Soft and hard tissue changes in Class III patients treated by bimaxillary surgery. Eur J Orthod. 1998; 20:25-33 https://doi.org/10.1093/ejo/20.1.25
Houston W, Jones E, James D. A method of recording change in maxillary position following orthognathic surgery. Eur J Orthod. 1987; 9:9-14 https://doi.org/10.1093/ejo/9.1.9
Jo L-J, Weng J-L, Ho C-T, Lin H-H. Three-dimensional region-based study on the relationship between soft and hard tissue changes after orthognathic surgery in patients with prognathism. PLoS One. 2018; 13 https://doi.org/10.1371/journal.pone.0200589
Lapatki B, Baustert D, Schulte-Mönting J, Frucht S, Jonas I. Lip-to-incisor relationship and postorthodontic long-term stability of cover-bite treatment. Angle Orthod. 2006; 76:942-949 https://doi.org/10.2319/090205-309
Dall'Magro A, Dogenski L, Dall'Magro E, Figur N, Trentin M, De Carli J. Orthognathic surgery and orthodontics associated with orofacial harmonization : Case report. Int J Surg Case Rep. 2021; 83 https://doi.org/10.1016/j.ijscr.2021.106013
Knowledge of the facial soft tissues is paramount with regard to orthodontic diagnosis, assessment and treatment planning. This paper will describe the relevance of extra- and intra-oral assessment of soft tissues, with a particular focus on the lips, in orthodontic diagnosis, treatment planning and potential treatment effects.
CPD/Clinical relevance: Knowledge of the extra-oral and intra-oral soft tissue assessment is important in the planning and execution of orthodontic treatment.
Article
Smiling is an innate and essential part of everyday communication. We know the position of the lips can be influenced by the underlying position of the labial segment teeth1. Similarly, the position of the lips may influence the positions of the teeth, both before and after orthodontic treatment. Therefore, there is a bidirectional relationship between the soft tissues of the lips and orthodontic outcome.
Research has shown that irregularities in the positions of the teeth can have a significant impact on smile aesthetics and, therefore, perceived attractiveness, quality of life and psychosocial wellbeing2. Orthodontic treatment may therefore result not only in changes to the position of the teeth and overlying soft tissues, but overall wellbeing.
This paper will discuss the relevance of the soft tissues, with a particular focus on the lips, in orthodontic diagnosis, treatment planning and potential treatment.
Extra-oral assessment
A comprehensive facial assessment includes analysis of the face and soft tissues, both in passive and animated states, with the lips being examined from the frontal and profile views. These assessments will be described in detail.
Lip anatomy
The lips comprise skin on their outer surface and lining mucosa on the inner surfaces. The lip skin contains the normal features found elsewhere in skin, such as sweat glands, sebaceous glands and hair follicles. The inner lining mucosa of the lips contains thick, non-keratinised epithelium with submucosa containing minor salivary glands. A highly specialised mucosa is present in the vermilion zone, the area of transition between the skin and the oral mucosa. The vermilion zone lacks mucous glands and sebaceous glands, hence the requirement for continuous moistening of the lips with saliva by the action of the tongue. The vermilion zone appears red due to the heavily vascularised papillae of the connective tissue projecting into the epithelium.
The muscles of facial expression are innervated by the facial nerve and are grouped around the orbit, ear, nose and mouth. Fibres of the orbicularis oris muscle pass around the lips and help to achieve lip closure and pursing. A number of other muscles are arranged radially from the orbicularis oris muscle and can be classified as superficial or deep muscles of the upper and lower lips. The levator labii superioris, for example, is a superficial muscle which elevates the upper lip. The depressor labii inferioris muscle depresses the lower lip. The buccinator muscle arises from the pterygomandibular raphe posteriorly. Most of its fibres insert into the mucous membrane of the cheeks, but some fibres intercalate with the orbicularis oris anteriorly.
Lip competence
The relationship of the lips can be viewed from both frontal and profile views, with the patient's lips relaxed. They can be classified as competent if they are together at rest, with minimal muscular effort required to achieve a lip seal.3,4 Conversely, lips are described as incompetent if they are apart at rest and require distinguishable muscular activity to form a lip seal.4 This muscular activity can be seen either through circumoral musculature contraction and straining of the lips,3 straining of the mentalis muscle resulting in visible ‘puckering’ of the chin or, alternatively, the patient might posture their mandible forward in order to obtain a lip seal.
Lip incompetence may be associated with either skeletal, dental or soft tissue discrepancies:
Skeletal – an antero-posterior skeletal discrepancy (e.g severe Class 2 pattern), vertical maxillary excess, or increased anterior facial height may contribute to lip incompetence directly, as the lips are not able to achieve closure due to the increased distance between the maxilla and mandible.
Dental – in the absence of any skeletal discrepancy, excessively proclined upper incisors may create a physical obstruction and lead to lip incompetence, often with an associated lower lip trap (Figure 1). In some cases, the lips may be described as being ‘potentially competent’, such that if the obstruction were removed, i.e. following retraction of the upper incisors, then the lips would easily be competent at rest.
Soft tissue – lip morphology itself, such as a short upper lip, or a low lower lip line,5 may also directly contribute to lip incompetence. Interestingly, the majority of pre-adolescent children have incompetent lips at rest, but lip competence tends to improve with age.6
Figure 1. At rest, this patient has incompetent lips with an associated lip trap as a result of excessively proclined upper incisors.
Lip length and incisor coverage
The average upper lip length is between 18–22 mm.7 Lip length differs between sexes, with males generally having longer upper lip lengths than females. The average upper lip length for Caucasian males is 21mm, and 20mm for females.8 Lip length and thickness increase until adolescence, after which the lips lengthen and become progressively thinner with age.9,10
Lip activity and lower lip line
In the case of a normal occlusion with Class I incisors, the lower lip will typically cover the incisal third of the upper incisors at rest. This is an average lower lip line.
In Class II division 2 incisor relationships, there is a tendency for the lower lip line to be higher. In this case, if the vertical position of the lower lip in relation to the upper incisors is high, then all four upper incisors will be retroclined. If the lip line is not as high, the upper central incisors might still be retroclined, but the upper lateral incisors, which are not in this case controlled by the lower lip, will typically be proclined, mesially angulated and mesiolabially rotated (Figure 2).
Figure 2. A Class II division 2 incisor relationship with a strap-like lower lip causing retroclination of the upper incisors. Note how the upper lateral incisors are not under the control of the lower lip and are proclined and mesiolabially rotated.
Additionally, lips which are strap-like with increased muscular activity can result in retroclination of either the upper or lower incisors, or both. This is most commonly associated with Class II division 2 incisor relationships.11
By contrast, flaccid lip tone or low lip pressure, is more likely to be associated with proclined incisors, either the upper incisors, or both the upper and the lower incisors. In the case of the latter, this can result in bimaxillary proclination and either a Class I or a Class II division 1 incisor relationship.11
Lip prominence and morphology
Lip prominence varies between ethnicities; Caucasian people tend to have relatively thin lips with minimal lip prominence, while people of Asian or African descent tend to have relatively thicker lips with greater lip prominence.12,13
Full, prominent, everted lip morphology is commonly associated with proclined incisors, and bimaxillary proclination is a relatively common presenting feature in Asian and African ethnic groups.
In the case of thin lips, flattening may occur with incisor retraction, which can have an undesirable effect on the facial profile, by making a person look more aged. In contrast, fuller lips may be able to mask some upper incisor retraction.9
In general, lip prominence or fullness is now regarded as a desirable feature of smile aesthetics, being associated with beauty and youth.14 Therefore, assessment of lip prominence and morphology should be taken into consideration if incisor retraction or extractions are part of the overall orthodontic treatment plan.
Nasolabial angle
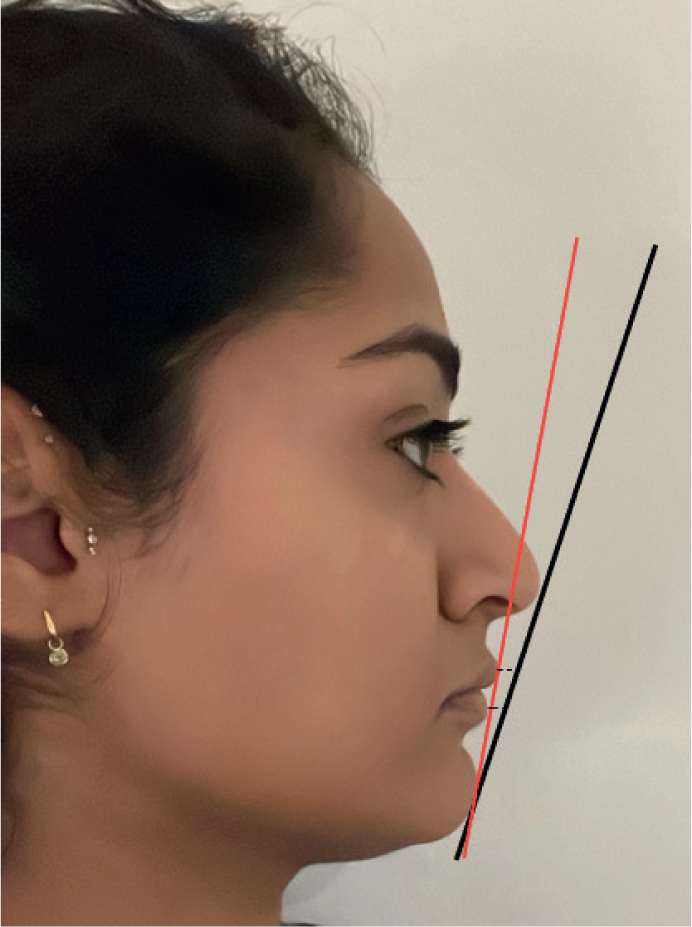
The nasolabial angle (NLA) is the angle created at the intersection of the ventral surface of the nose and labial surface of the upper lip (Figure 3). In the literature, the normal values range from 90–120°,15 but there are variations across ethnicities, as well as between males and females (Table 1). Compared to Caucasian norms, people of African and East or Southeast Asian descent tend to have a more acute NLA.16
Figure 3. Black line depicts nasolabial angle. Yellow line depicts labiomental angle. Both measurements are average in the case of this patient.
Table 1. Variations in nasolabial angle (NLA) between males and females across different ethnicities. Adapted from Wen et al, 2015,16 with mean values rounded to nearest whole number.
African
Asian
Caucasian
Average NLA (males)
88°
95°
100°
Average NLA (females)
86°
94°
103°
An increased NLA can occur with a relatively normal upper lip position if the columella of the nose slopes upwards (an upturned nose). A decreased NLA can occur if the upper lip is protrusive, but may also occur where the upper incisors are particularly proclined or when the use of lip fillers has caused the lips to appear fuller and more protrusive.
The NLA is influenced by changes in the anteroposterior position and inclination of the lip. Therefore, the profile of the nose and the NLA should be considered when planning treatment, especially when the general consensus within orthodontics is that retraction of incisors, in certain patients, increases the NLA.17,18 In some cases, acceptance of an increased overjet at the end of treatment may need to be considered, to avoid detrimental changes to the facial profile if further retraction is required to reduce the overjet fully.
Labiomental angle
The labiomental angle is the angle formed between the lower lip and chin, and normal values range from 110–130°.7 When describing the labiomental angle, orthodontists are often referring to the labiomental fold (Figure 3). This can be influenced by lower incisor inclination, as well as the shape of the chin. If the lower incisors are excessively proclined, then the labiomental angle is decreased. A prominent chin point may also be associated with a decreased angle. Research investigating the aesthetics of the labiomental angle found that an angle of between 107–118° was deemed to be the most attractive, and deep labiomental folds (decreased angles) or shallow folds (increased angles) the least attractive.19
Intra-oral assessment
It is important to know that even in animated states, there is a difference between a posed smile, and a spontaneous smile. This concept was first appreciated by Leonardo da Vinci.20
A posed, or social smile, is the commonly used smile in day-to-day life that is routinely presented to the world. It is fairly easy to elicit a posed smile, for example by asking someone to smile for a photograph. Posed smiles are voluntary and not linked with emotion and, as a result, are reproducible to a certain degree (Figure 4).
Figure 4. Posed smile.
On the other hand, a spontaneous smile (Figure 5), also known as a Duchenne smile or ‘enjoyment smile’, is involuntary and linked with emotion.21 The Duchenne smile, identified by the French neurologist Guillaume Duchenne in the mid 19th century, involves the zygomaticus major and orbicularis oculi muscles. This type of smile is considered to be a display of genuine happiness, involving activation of the eyes, sometimes causing the creation of crow's feet. Obtaining this smile requires a little more effort, and can be achieved if someone is made to laugh.
Figure 5. The same patient in Figure 4 but with a spontaneous smile. Note the activation of the eyes and creation of crow's feet, along with increased tooth and gingival show due to activation of the zygomaticus major muscles and superficial muscles of the upper lip.
Overall, it is the posed or social smile that should be the focus in orthodontic diagnosis, as it is the most commonly encountered smile, and the most reproducible.
Ideal smile aesthetics – the relationship between upper lip line, incisors and gingival display
The upper lip line is the vertical relationship between the upper lip and upper incisors. It has an influence on the amount of incisor and gingival display and is dependent on whether the lips are at rest or active, such as during smiling. The upper lip line is influenced by lip length, which will alter with age. Generally, after the age of 30 years, the amount of incisal display reduces as the upper lip lengthens and drapes further over the maxillary anterior teeth.22 It is important to remember this change in the relationship of the lips to the teeth will occur after adolescence.
It has been shown that people with ideal upper lip lines, and therefore pleasing smile aesthetics, have around 2-4 mm of upper incisor show at rest,23,24 with males showing less tooth than females on average. If the values fall outside of this range the smile is deemed less attractive.
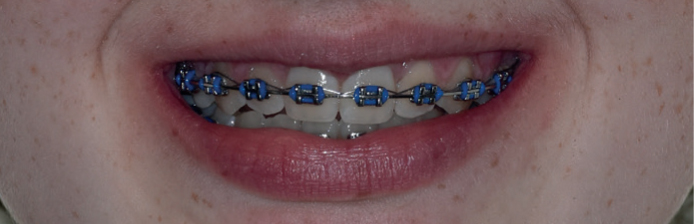
On smiling, the full height, or 100% of the upper incisor crowns, plus interdental papillae should normally be visible, with some gingival show being deemed acceptable (Figure 6). However, more recently it has been suggested, with the social smile at least, that a minimum 75% of the full height of the central incisor should be displayed.25 Therefore, optimum aesthetics would dictate 75–100% of the upper incisor crowns being visible on smiling. Females tend to have a higher upper lip line (by 1–2mm) in comparison to males, and therefore it is generally acceptable for females to show 1–2 mm more coronal height and gingival tissue than males.
Figure 6. Social smile showing between 75% and 100% of the upper incisor crowns, as well as interdental papillae.
A low upper lip line results in reduced incisor display (i.e. with less than 75% of the upper incisor crown height on smiling) and can be deemed unattractive (Figure 7). By contrast, a high upper lip line can result in excessive gingival display (see Figure 8), and a ‘gummy’ smile, which is where a continuous band of gingival tissue is visible, which can result in undesirable smile aesthetics (Figure 8).26 It can be indicative of short clinical crowns, vertical maxillary excess, a short upper lip or a hypermobile upper lip resulting in excessive lip elevation on smiling.
Figure 7. Social smile showing around 50% of the upper incisor crowns, and no interdental papillae.Figure 8. Excessive gingival show as a result of vertical maxillary excess and high upper lip line.
Although a large gummy smile is considered unattractive, it is worth remembering that a slight gummy smile in adolescence may look ideal in adulthood, as the upper lip length increases with age. This should be factored in during orthodontic diagnosis and treatment planning.
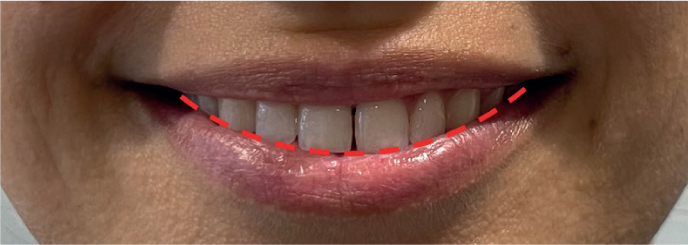
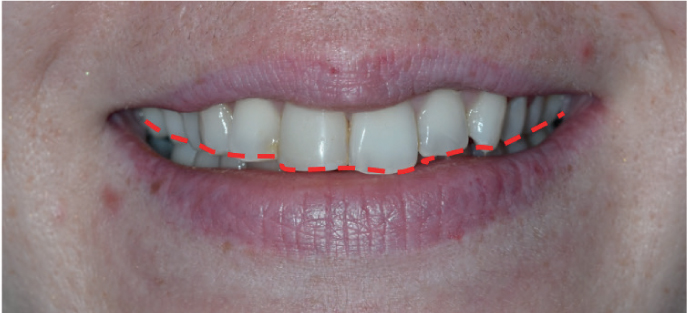
Smile arc
The smile arc is the contour of the upper incisal edges relative to the curvature of the lower lip when producing a social smile, and is regarded as an important determinant of the attractiveness of a smile.27 The relationship between the edges of the upper incisors and the curvature of the lower lip should be parallel on smiling (Figure 9), and this is known as a consonant smile arc. Flattening of the smile arc, or a non-consonant smile arc (Figure 10), can make a smile look aged (as older individuals often have tooth wear which flattens the arc of the teeth), and will result in poorer smile aesthetics in both males and females.
Figure 9. A consonant smile arc.Figure 10. A non-consonant smile arc.
Buccal corridors and smile width
A dimension of recent interest in dentistry is the amount of buccal corridor displayed on smiling (Figures 11 and 12). Buccal corridors are defined as the space between the upper posterior teeth (especially the premolars) and the inside of the cheek. The ideal amount of black space of intercommissure width is said to be approximately 6–26.5%,25,28 with this value being calculated from the total dark space on both sides of the mouth as a percentage of the total smile width.25 It is therefore important to take into account the transverse dimension of the maxillary arch when assessing the patient, alongside the axial inclinations of the buccal segment teeth.
Figure 11. Average smile width with average-sized buccal corridors.Figure 12. Broad smile with no buccal corridors.
While narrow maxillary arches and wide buccal corridors are deemed unaesthetic, it is important not to over-broaden a smile, as this can tend to look artificial, and is likely to be unstable. Similarly, patients who have posterior teeth which are already buccally flared may not be good candidates for expansion or broadening the smile. The exception to this would be correction of a unilateral crossbite with a displacement, where the increase in inter-canine and inter-molar width is necessary to address the malocclusion.29
Special investigations
Cephalometric analysis
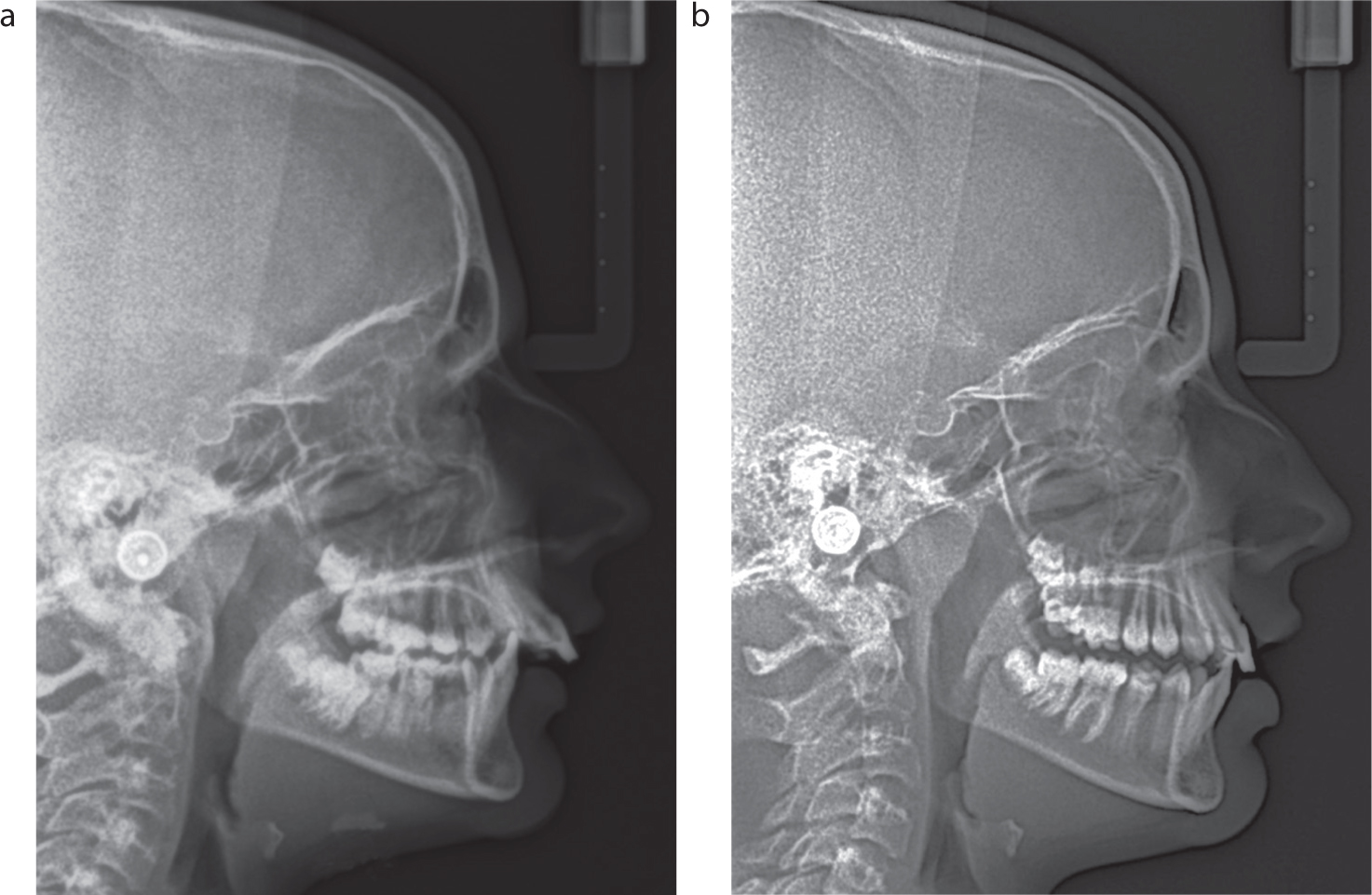
Clinical examination of the soft tissues can be supported by lateral cephalometric radiographs, with several soft tissue analyses being available to allow a more detailed orthodontic assessment. However, a limitation of cephalometric radiography is that the position of the lips may not be at rest during exposure and, as such, may influence the resulting cephalometric analysis (Figure 13).
Figure 13. Lateral cephalometric radiographs of the same patient showing lips apart, which may influence the resulting soft tissue analysis. (a) Note that the lips were likely apart due to the increased overjet. (b) The teeth were not in occlusion as patient was post-functional appliance therapy.
Holdaway analysis and H-line
The Holdaway soft tissue analysis is a complex analysis, with 11 points required for quantifying facial harmony and soft tissue balance.30,31 It evaluates the relationship between hard and soft tissues, and how the latter may respond to orthodontic treatment. With regards to the soft tissue response, Holdaway himself stated that some patients' faces looked better before the orthodontic corrections were made.
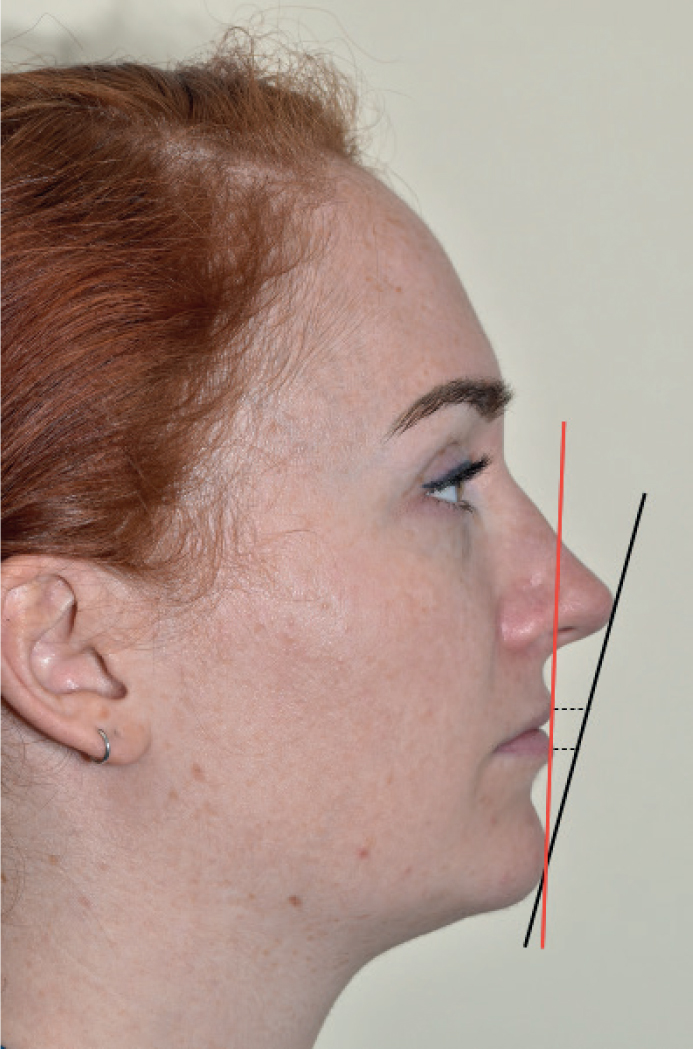
The analysis addresses the main characteristics of the mid and lower facial thirds, including measurements for the soft-tissue facial angle, upper and lower lip thicknesses and sulcus depths, and nose prominence. The Holdaway line, or simply the H-line, is a line drawn from the most prominent point of the upper lip to the soft tissue of the chin (Figures 14 and 15). In an average face, this line should bisect the nose. However, the analysis was based upon Caucasian patients and so is not valid or generalisable to the entire population.
Figure 14. The Holdaway line (red), and Rickett's E-line (black), with dotted lines drawn at a tangent to demonstrate relative anteroposterior positions of upper and lower lips.Figure 15. The Holdaway line (red), and Rickett's E-line (black) – note how the Holdaway line bisects the nose closer towards the tip in this non-Caucasian individual compared to Figure 14.
Rickett's E-Line
Rickett's E-Line, where the ‘E’ stands for ‘esthetic’, can be used to assess lip fullness and the position of the lips relative to the facial profile. This line can be used both cephalometrically and clinically. The line is drawn from the tip of the nose to the chin point (Figures 14 and 15). The upper lip should lie 4mm behind this line, and the lower lip should lie 2mm behind this line. If the lower lip lies ahead of this line, it is considered protrusive, and if it lies more than 2mm behind the line, it is considered retrusive. The line can be affected by the prominence of the nose, with a more anteriorly displaced line seen with a larger nose, and so care must be taken when assessing the lips.
Three-dimensional imaging
Conventional 2D imaging, such as in radiographs and photographs, involve only two axes (the vertical y and horizontal x axes). In contrast, the Cartesian coordinates system of three-dimensional (3D) imaging involve the x, y, and z axes, which are the transverse, vertical and anteroposterior or ‘depth’ axes respectively.32 3D imaging techniques such as laser scanning and stereophotogrammetry are popular due to their obvious advantages of posing no radiation risk to the patient, and they allow a 3D image of the face to be viewed and manipulated in any direction.
Laser scanning provides a non-invasive method of capturing the soft tissues of the face for treatment planning. However, this method is fairly slow, requiring a long capture time, making it less suitable for young patients who may not be able to sit still for long enough. There are also potential safety issues with regards to the laser beam and the eyes and the final 3D image is viewed in single colour.
Unlike laser scanning, stereophotogrammetry involves a pair of configured cameras taking simultaneous photographs of the facial region, and combining the images taken from the two different directions to create a 3D image33. Not only does the short capture time make it suitable for use with younger patients, but the images created are rendered in full colour 3D.
Predicting soft tissue changes following treatment
Extractions
There is some controversy within orthodontics about whether extractions alter the facial profile. A study which analysed 3D facial scans of a group of patients who underwent extractions compared to those with no extractions, found that orthodontic treatment involving extractions did not have a detrimental effect on the face.34 However, a systematic review found that premolar extractions can increase the nasolabial angle by 2.4–5.4 degrees.35 A further systematic review and meta-analysis found that the NLA was significantly increased when premolar extractions were part of the orthodontic treatment plan, compared to non-extraction based treatment plans.18 However, it has been reported that the soft tissue response is often unpredictable following extractions and incisor retraction,18,36 so it is advisable to make decisions on an individual case-by-case basis.
Orthognathic surgery
A malocclusion associated with a significant skeletal discrepancy of a non-growing patient will often require a combination of orthodontics and orthognathic surgery to reposition the jaws for definitive correction. Achieving a harmonious facial appearance is often a key motivation for patients. Therefore, it is important that the treatment planning process includes evaluation of the anticipated soft tissue changes with surgical repositioning of the dentofacial skeleton.
Factors related to surgery, such as post-operative oedema and swelling, are inevitable and will affect the soft tissue response, but these are often difficult to control or predict and vary between individuals.37 Additionally, the prediction of soft tissue changes has been found to be less accurate for bimaxillary surgeries than for single jaw surgeries.38 For example, changes to the nasal tip and nasolabial angle, as well as broadening of the alar base can be seen in conjunction with maxillary surgery.39,40 Attempts to counteract alar base widening, including the incorporation of techniques such as the alar base cinch suture, can also lead to unintended increases in nasal tip elevation and overall increase in nasolabial angle in the short-term. In the long-term, these changes often resolve,41 but this further demonstrates the inherent unpredictability of the soft tissues not only intra-operatively, but also post-operatively.
The soft tissues of the face do not respond in a linear manner following alteration of the underlying hard tissues.42 The soft tissue response is variable due to differences in soft tissue thickness, tonicity of musculature, variations in the amount of bone removal and destruction of bony landmarks.43,44
Cephalometrics can be used to attempt to predict the soft tissue response to surgery, but this is prone to error due to the difficulty in identifying both hard and soft tissue landmarks on 2D anatomical structures.45 Some cephalometric programmes, such as Dolphin (Dolphin Imaging & Management Solutions; California, USA) allow for 3D soft tissue predictions with the software using a landmark-based photographic morphing algorithm that was originally developed for 2D prediction, and later adapted for 3D prediction.42 This transfer of 2D data to a 3D representation may explain some of the errors and inaccuracies in a programme-based soft tissue prediction. Although cephalometric planning and prediction may help to guide clinicians and counsel patients on likely treatment outcomes, these are only a guide and do not accurately depict the actual surgical outcome. Care should therefore be exercised in providing pre-operative orthognathic patients with soft tissue predictions for any planned surgery.
Influence of the lips on stability
If the lips play a role in the aetiology of a malocclusion, then the lips should be considered when determining the likely stability of a treated malocclusion.
Two good examples of this can be seen with Class II division 1 and Class II division 2 incisor relationships. In a Class II division 1 incisor relationship, on a Class I or mild Class II skeletal base, where there is a lower lip trap leading to proclination of the upper incisors, if the upper incisors are retracted to a position where they are under the control of the lower lip, they are less likely to procline and therefore relapse after treatment.
In the case of a Class II division 2 incisor relationship with a high lower lip line causing retroclination of the upper incisors (Figure 2), a principal treatment objective would be to intrude the upper incisors to a more normal relationship with the lower lip (Figure 16). This will remove the excessive overlap of the upper incisors by the lower lip, which might otherwise lead to retroclination and relapse.46
Figure 16. The same patient from Figure 2, who is nearing completion of orthodontic treatment. Note how the upper incisors have been intruded relative to the lower lip, which is also evident by reduced gingival show
Lip augmentation and dermal fillers
The growing trend in the use of dermal fillers for augmentation of the soft tissues of the face, particularly the lips, means it is worthwhile to consider lip fillers in relation to orthodontic assessment.
The aesthetic injectables market has recently been growing by more than 10% a year, and the industry is estimated to be worth approximately £2.75 billion in the UK.47 As these are becoming increasingly commonplace in the world of dentistry, it is important to ask patients about any non-surgical procedures, such as the use of dermal fillers, when taking an orthodontic history.
There are instances where injectable fillers can be used appropriately to harmonise facial proportions,48 and in certain cases, can be a suitable non-surgical option for facial augmentation. If these have been used, then the clinician should keep in mind that the facial proportions will not be accurately represented during the soft tissue assessment. Therefore, working to pre-augmentation proportions with the use of patient photographs should be considered where possible. This is particularly relevant during orthognathic planning, as patients may have attempted to alter their soft tissue profile prior to planned orthognathic surgery.49 Such patients may be keen to camouflage their skeletal pattern with the use of dermal fillers in the lips, nose or chin. However, they may later seek a combined orthodontic-orthognathic approach to address the skeletal discrepancy. In such instances, restoration of the soft tissues to their original form, which may involve dissolving of dermal fillers, where possible, may be required.
Conclusions
In the context of orthodontic treatment planning, the lips play an important role in the aetiology and successful treatment of a malocclusion. Consideration should not only be given to the lips in isolation, but also their relationship to the teeth, the gingivae and other important facial structures, allowing ideal facial and smile aesthetics to be achieved. This is paramount for attaining an excellent patient outcome with improved stability.