Krishnan V, Davidovitch Z Biological basis of orthodontic tooth movement, 3rd edn. In: Krishnan V, Kuipers-Jagtmana AM, Davidovitch Z (eds). : Wiley; 2021
Meikle MC The tissue, cellular, and molecular regulation of orthodontic tooth movement: 100 years after Carl Sandstedt. Eur J Orthod. 2006; 28:221-240 https://doi.org/10.1093/ejo/cjl
Krishnan V, Davidovitch Z Cellular, molecular, and tissue-level reactions to orthodontic force. Am J Orthod Dentofacial Orthop. 2006; 129:469.e1-32 https://doi.org/10.1016/j.ajodo.2005.10.007
Masella RS, Meister M Current concepts in the biology of orthodontic tooth movement. Am J Orthod Dentofacial Orthop. 2006; 129:458-468 https://doi.org/10.1016/j.ajodo.2005.12.013
Kong YY, Yoshida H, Sarosi I OPGL is a key regulator of osteoclastogenesis, lymphocyte development and lymph-node organogenesis. Nature. 1999; 397:315-323 https://doi.org/10.1038/16852
Bucay N, Sarosi I, Dunstan CR Osteoprotegerin-deficient mice develop early onset osteoporosis and arterial calcification. Genes Dev. 1998; 12:1260-1268 https://doi.org/10.1101/gad.12.9.1260
Sandy JR, Farndale RW, Meikle MC Recent advances in understanding mechanically induced bone remodeling and their relevance to orthodontic theory and practice. Am J Orthod Dentofacial Orthop. 1993; 103:212-222 https://doi.org/10.1016/0889-5406(93)70002-6
Kehoe MJ, Cohen SM, Zarrinnia K, Cowan A The effect of acetaminophen, ibuprofen, and misoprostol on prostaglandin E2 synthesis and the degree and rate of orthodontic tooth movement. Angle Orthod. 1996; 66:339-349
Bradley RL, Ellis PE, Thomas P A randomized clinical trial comparing the efficacy of ibuprofen and paracetamol in the control of orthodontic pain. Am J Orthod Dentofacial Orthop. 2007; 132:511-517 https://doi.org/10.1016/j.ajodo.2006.12.009
Ireland AJ, Ellis P, Jordan A Comparative assessment of chewing gum and ibuprofen in the management of orthodontic pain with fixed appliances: a pragmatic multicenter randomized controlled trial. Am J Orthod Dentofacial Orthop. 2016; 150:220-227 https://doi.org/10.1016/j.ajodo.2016.02.018
Monk AB, Harrison JE, Worthington HV, Teague A Pharmacological interventions for pain relief during orthodontic treatment. Cochrane Database Syst Rev. 2017; 11 https://doi.org/10.1002/14651858.CD003976.pub2
Deng Y, Sun Y, Xu T Evaluation of root resorption after comprehensive orthodontic treatment using cone beam computed tomography (CBCT): a meta-analysis. BMC Oral Health. 2018; 18 https://doi.org/10.1186/s12903-018-0579-2
Kaley J, Phillips C Factors related to root resorption in edgewise practice. Angle Orthod. 1991; 61:125-132
Yassir YA, McIntyre GT, Bearn DR Orthodontic treatment and root resorption: an overview of systematic reviews. Eur J Orthod. 2021; 43:442-456 https://doi.org/10.1093/ejo/cjaa058
Unsterseher RE, Nieberg LG, Weimer AD, Dyer JK The response of human pulpal tissue after orthodontic force application. Am J Orthod Dentofacial Orthop. 1987; 92:220-224 https://doi.org/10.1016/0889-5406(87)90415-x
Derringer KA, Jaggers DC, Linden RW Angiogenesis in human dental pulp following orthodontic tooth movement. J Dent Res. 1996; 75:1761-1766 https://doi.org/10.1177/00220345960750100901
Weissheimer T, Silva EJNL, Pinto KP Do orthodontic tooth movements induce pulp necrosis? A systematic review. Int Endod J. 2021; 54:1246-1262 https://doi.org/10.1111/iej.13523
Singh A, Varma AR Whole-body vibration therapy as a modality for treatment of senile and postmenopausal osteoporosis: a review article. Cureus. 2023; 15 https://doi.org/10.7759/cureus.33690
DiBiase AT, Woodhouse NR, Papageorgiou SN Effects of supplemental vibrational force on space closure, treatment duration, and occlusal outcome: a multicenter randomized clinical trial. Am J Orthod Dentofacial Orthop. 2018; 153:469-480.e4 https://doi.org/10.1016/j.ajodo.2017.10.021
Frost HM The regional acceleratory phenomenon: a review. Henry Ford Hosp Med J. 1983; 31:3-9
Mheissen S, Khan H, Alsafadi AS, Almuzian M The effectiveness of surgical adjunctive procedures in the acceleration of orthodontic tooth movement: a systematic review of systematic reviews and meta-analysis. J Orthod. 2021; 48:156-171 https://doi.org/10.1177/1465312520988735
Chachartchi T, Itai Y, Tzach-Nahman R Mechanical force application and inflammation induce osteoclastogenesis by independent pathways. Clin Oral Investig. 2023; 27:5853-5863 https://doi.org/10.1007/s00784-023-05196-8
Yashin D, Dalci O, Almuzian M Markers in blood and saliva for prediction of orthodontically induced inflammatory root resorption: a retrospective case controlled-study. Prog Orthod. 2017; 18 https://doi.org/10.1186/s40510-017-0176-y
Huang GY, Choi SH, Jung HD Tissue-specific biomarkers in gingival crevicular fluid are correlated with external root resorption caused by constant mechanical load: an in vivo study. Clin Oral Investig. 2021; 25:6321-6333 https://doi.org/10.1007/s00784-021-03932-6
Coordinated biological responses are required to bring about orthodontic tooth movement. Several theories have been proposed for the mechanisms underlying tooth movement. Techniques have been investigated for reducing pain associated with orthodontics, as well as increasing the rate of tooth movement. Modern molecular and genetic techniques have improved our understanding of biological processes underlying tooth movement, but there is still a great deal of detail that is unknown.
CPD/Clinical Relevance: This article provides an update on contemporary theories of orthodontic tooth movement.
Article
Teeth have been moved orthodontically in humans for centuries. The idea of bone resorption being the method by which teeth move through bone when an orthodontic force is applied was proved by Sandstedt in the early years of the 20th century, with the publication of a report of the histology of orthodontic tooth movement.1 Research continued throughout the 20th century using histological techniques, but also increasingly, molecular biology and molecular genetics. An important review of the mechanisms regulating orthodontic tooth movement was published by Meikle in 2006 when he stressed that a three-dimensional perspective is essential for understanding the biological events regarding tooth movement and that the process includes deflection of alveolar bone and concurrent remodelling of periodontal tissues.2
Orthodontists across the world rely on the biological processes underlying tooth movement through bone. Understanding that orthodontic tooth movement relies on coordinated responses within the bone and the periodontal ligament of teeth is important for clinical care and also has implications for development of new techniques.
Historical theories of orthodontic tooth movement
Several theories have been proposed for the mechanisms underlying orthodontic tooth movement. An empirical known is that mechanical stimuli bring about cellular responses resulting in tooth movement.
Bone bending
Several parallels have been drawn in the past regarding the bony resorption and deposition that occurs during tooth movement with the activity of long bones, which respond with either bone resorption or formation when bones are bent. By applying pressure to teeth, it was thought that bone bending occurs, resulting in bone turnover and resorption and deposition.
Pressure–tension hypothesis
If the periodontal ligament is regarded as a closed system, then differential pressures within the system may contribute to the alveolar bone remodelling around the tooth. It was thought that periodontal ligament fibres may be able to transfer orthodontic forces directly into the bone. This theory has been discounted because the periodontal ligament is likely to act as a continuous hydrostatic system, where any forces are likely to be distributed evenly throughout the system. Moreover, if the integrity of the periodontal ligament is compromised with drugs that disrupt collagen cross linking, teeth will still move with the application of orthodontic forces.
Piezo-electric forces
It has been observed that bending bone can result in electrical effects. Two types of effects have been observed. Distortion of fixed structures can result in piezo-electric potentials, whereas streaming potentials are prevalent in hydrated tissues. It was thought that these stress-generated electrical effects were responsible for bony remodelling. It is more likely that these electrical effects were a chance observation and not important for the causation of bone remodelling.3
Meikle's overview was instrumental in summarizing that orthodontic tooth movement is the result of mechanotransduction events resulting in a feedback mechanism causing the synthesis of cytokines (cell signalling molecules) by osteoblast cells.2 These in turn result in regulation of expression of transcription factors, cytokines and growth factors, causing differentiation and proliferation of other cell types.
Bone biology
Bone consists primarily of hydroxyapatite mineral (70%) in a scaffold of type I collagen (27%). The remaining components of bone consist of glycosaminoglycans, other minor collagen types and other proteins, including osteocalcin, osteonectin, osteopontin and glycoproteins. Bone matrix also contains polypeptide growth factors, bound to proteins. The cellular component of bone (osteoblasts, osteocytes and osteoclasts), although only a small proportion of bone's total volume, is instrumental in facilitating bone development and turnover.
Osteoblasts
Osteoblasts are large cells that synthesize and maintain the collagenous matrix. They are derived from mesenchymal cells and undergo a differentiation process to change from immature pre-osteoblasts into functional, mature osteoblasts. When bone is growing, the osteoblasts are cuboidal in shape and proliferate. As well as producing type I collagen, the osteoblasts also facilitate mineralization of the matrix, by attracting accumulation of calcium and phosphate ions.
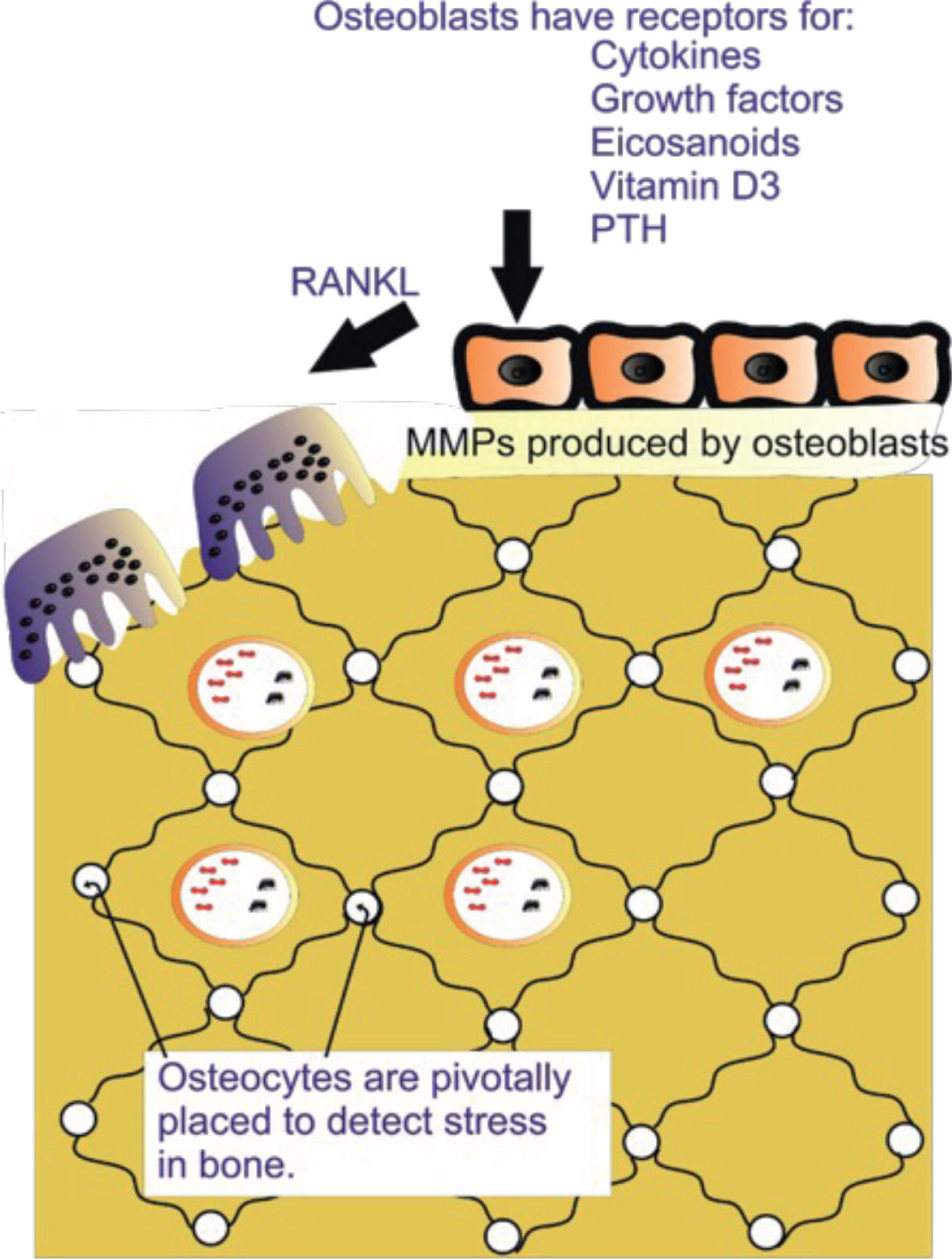
Osteoblasts have receptors for parathyroid hormone and cytokines, and they are instrumental in recruiting and activating osteoclasts in response to the environment. When stimulated in response to bone-seeking hormones, osteoblasts produce matrix metalloproteinases that help to degrade the collagenous osteoid (unmineralized bone) layer, facilitating access to the bone for osteoclasts.
Osteocytes
When osteoblasts have produced sufficient bone matrix, they essentially become enclosed within the bone and are terminally differentiated. These cells then become known as osteocytes. Small channels, or canaliculi, allow communication between the cells, as well as providing nutrients for cell survival. The channels of communication allow osteocytes to detect distortions of the bone caused by mechanical forces.
Osteoclasts
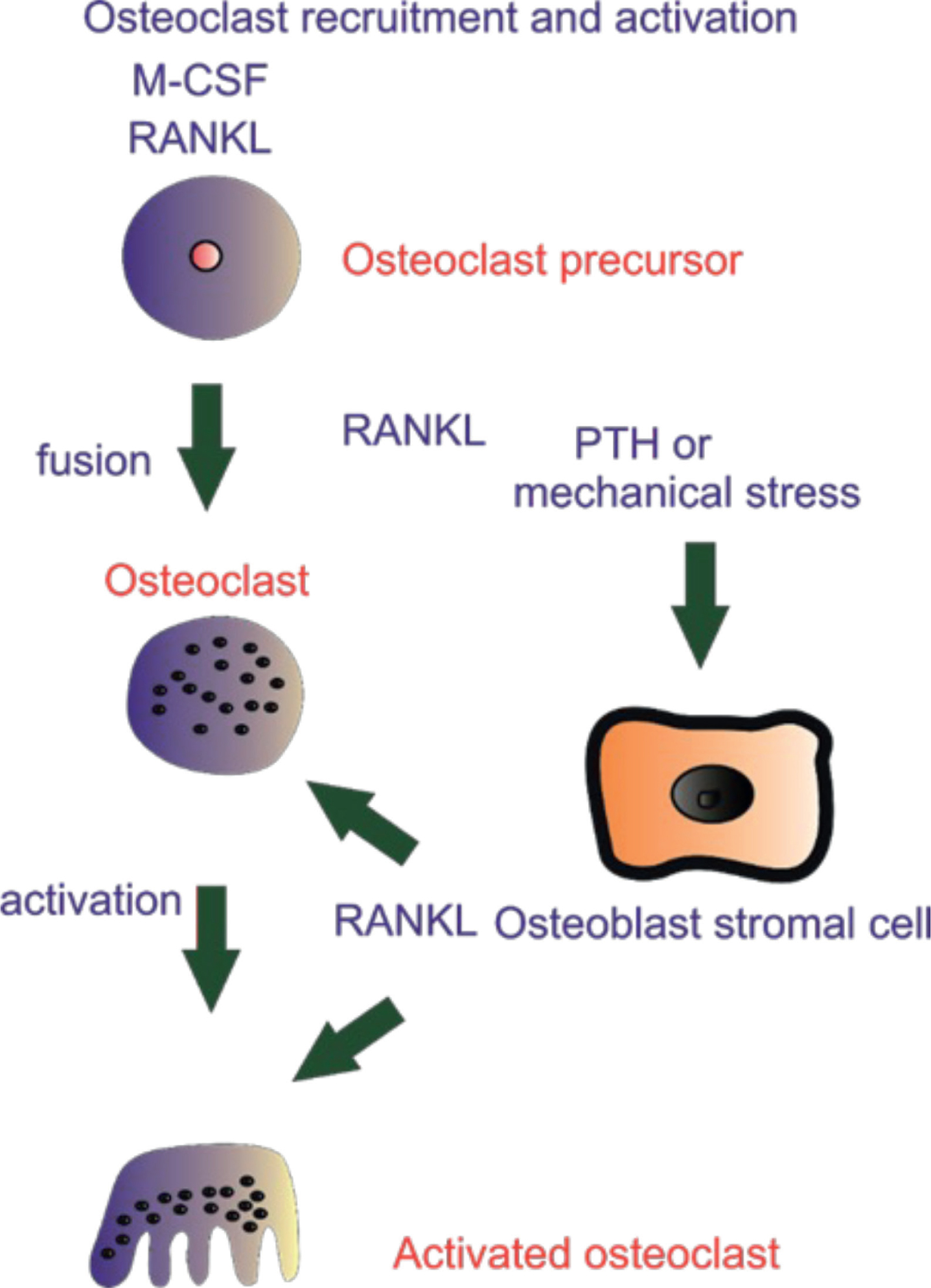
Osteoclasts are large multinucleated cells that are derived from monocytes in the blood. They are responsible for bone resorption. The cytoplasm of osteoclasts is highly active and facilitates dissolution of bone by creating an acid environment, alongside proteolytic enzymes, to resorb the bone in the localized environment. Osteoclasts only become activated by signals from osteoblasts. Osteoclasts have relatively few receptors on their surface compared to osteoblasts and these receptors tend to have inhibitory activity, whereby activation of the receptor results in a decrease in osteoclastic activity.
Interactions between osteoblasts and osteoclasts
The interactions between osteoblasts and osteoclasts are key to understanding the biology of orthodontic tooth movement. Osteoblast and osteoclast relationships have been described as ‘sensitive environment-to-genome-to-environment communicators’ orchestrating the bone response.4
Osteoclastic function is regulated by osteoblasts, via the osteoprotegerin/receptor activator of nuclear factor ligand/receptor activator of nuclear factor (OPG/RANKL/RANK) system.5 Osteoclasts in isolation do not resorb bone and require prior activation by osteoblasts. RANK receptors are present on the cell membrane of osteoclastic precursors. RANKL is a soluble factor secreted by osteoblasts that stimulates differentiation and activation of osteoclastic cells. RANKL activation of the osteoclasts is therefore required for bone resorption (Figures 1 and 2). There is regulation of this system by OPG. The latter is secreted by osteoblasts and binds to RANKL in the extracellular environment. OPG therefore has a protective effect on bone, as can be inferred from the name, ‘osteoprotegerin’. This key regulatory pathway was deduced from research using a genetically manipulated mouse model, where OPG-deficient mice developed severe bone porosity and a high incidence of bony fractures, consistent with osteoporosis. Mice overexpressing OPG showed increased bone density, essentially becoming osteopetrotic.6
Figure 1. Bone biology. Osteocytes detect distortion of bone caused by mechanical forces. Osteoblasts have receptors for cytokines and parathyroid hormone (PTH). When stimulated, osteoblasts produce receptor activator of nuclear factor ligand (RANKL), stimulating osteoclastic activation. The osteoblasts also produce matrix metalloproteinases (MMPs), facilitating removal of unmineralized bone to allow osteoclastic access to the mineralized bone.Figure 2. Osteoclastic recruitment and activation. Osteoclasts are large multinucleated cells, derived from monocytes in the blood. They are activated by receptor activator of nuclear factor ligand (RANKL) produced by osteoblast. M-CSF: macrophage colony stimulating factor; PTH: parathyroid hormone.
Matrix regulation
Prior to osteoclastic removal of calcified matrix within the bone, the thin layer of osteoid (unmineralized bony matrix) covering the bone must be removed to allow osteoclastic access. This process occurs when matrix metalloproteinase (MMPs) enzymes digest the components of the connective tissue, such as collagen. The MMPs are produced by stimulated osteoblasts. The activity of this group of enzymes is regulated by a group of inhibitors known as tissue inhibitors of metalloproteinases (TIMPs).
The biology of orthodontic tooth movement
Orthodontic tooth movement is based around the concept that mechanical stimuli are transmitted into and through bone to produce a response which results in tooth movement.
Application of force to cell membranes is now known to trigger internal cellular processes and second messengers, effectively converting the external stimulus into internal signals, ultimately resulting in changes in the nucleus of the cell. These nuclear responses result in production of either bone-resorbing factors, which recruit and activate osteoclasts, or bone-forming growth factors.
The force application to the cell membrane causes activation of the enzyme, phospholipase A2, which acts on the phospholipid cell membrane to release arachidonic acid. This becomes metabolized by two enzyme pathways, the cyclo-oxygenase (COX) and lipoxygenase (LOX) pathways. COX and LOX pathways produce prostaglandins and leukotrienes. Prostaglandins and leukotrienes activate some second messenger systems within cells, namely cAMP, inositol phosphates and tyrosine kinases.
The cytoskeleton of a cell is the network of filaments that supports the cell shape. The cytoskeleton is linked to the extracellular environment by transmembrane receptors, known as integrins. If the extracellular matrix is distorted, the integrins are activated and connect to the intracellular cytoskeleton, resulting in the transduction of the mechanical stimulus into a cellular response.7 These cellular responses can vary, but may include expression of cytokines and growth factors, causing differentiation and proliferation of other cell types in the region, hence causing the bone turnover process to start. These cellular responses take time, hence why bone remodelling is not instantaneous upon initial application of orthodontic force. It is thought that the cellular reactions last approximately 2–3 days prior to the initiation of bone remodelling.
Ideal orthodontic forces
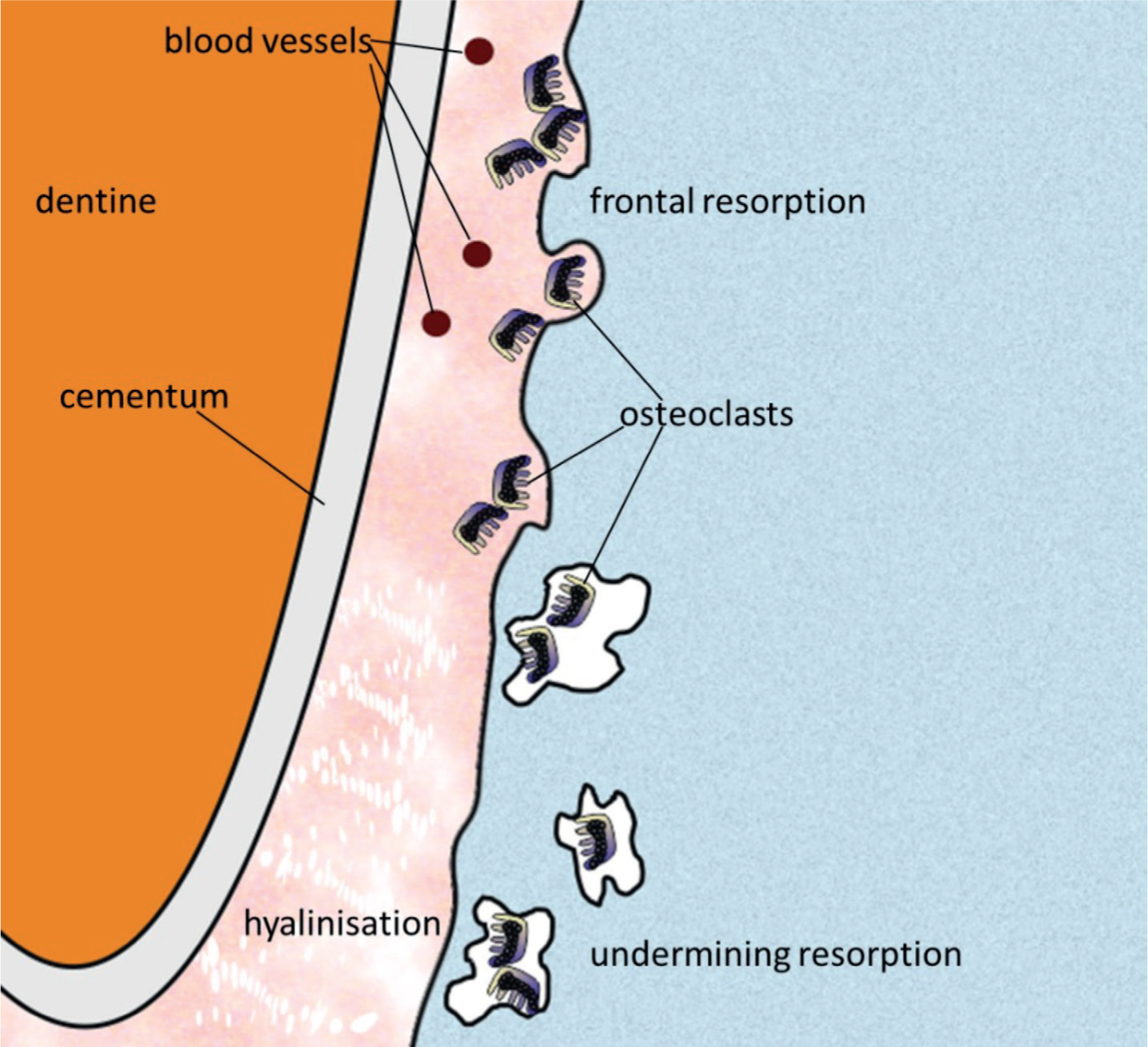
Ideal orthodontic forces have been proposed to be below that of capillary pressure (15–35mmHg), which is said to result in frontal resorption. This is tooth movement associated with light forces when bone is resorbed on the pressure side of the tooth and the osteoclasts are derived from the blood vessels within the periodontal ligament.
If the tooth movement forces are above that of capillary pressure, i.e. above 35mmHg, then tissue necrosis occurs and the process of undermining resorption. The periodontal ligament is described as ‘glass-like’ or hyalinized and the osteoclastic activity is not in the periodontal ligament, but from within the bone, therefore being described as undermining resorption (Figure 3). This type of tooth movement is likely to be painful. True frontal resorption is unlikely to happen at all points in the periodontal ligament at all times. It is much more likely that there will be areas of frontal resorption and areas of undermining resorption as the tooth moves.
Figure 3. Frontal and undermining resorption. Tooth movement forces below capillary pressure result in frontal resorption. Forces above capillary pressure result in undermining resorption.
Pain and orthodontic tooth movement
Pain associated with orthodontic tooth movement has been reported by most patients to start 2 hours after placement of appliances and peak at 24 hours. The pain usually subsides over a 5–7-day period, although as any orthodontist will report, there seems to be a wide range of experience.8,9
The pain experienced during orthodontic tooth movement is likely to be due to the inflammatory reactions in the periodontium and dental pulp. When there is vascular compression within the periodontium, the cells of the periodontal ligament, predominantly fibroblasts, undergo anaerobic respiration which causes local acidosis. The hydrogen ions bind sensory endings generating pain. Mast cells and fibroblasts release inflammatory mediators, including prostaglandins and bradykinin, which bind to sensory endings also generating the sensation of pain. This process occurs concurrently with osteoclastic bony remodelling. Neurogenic mediators such as calcitonin gene-related peptide (CGRP) and substance P (SP) are also generated.10
Various pain management techniques have been proposed for reducing pain associated with orthodontic tooth movement, including both pharmacological and non-pharmacological techniques.
Common analgesics recommended for orthodontic pain are paracetamol and ibuprofen. Paracetamol is an analgesic and antipyretic. Its mode of action is thought to be weak inhibition of prostaglandin synthesis and also a central analgesic effect. Ibuprofen causes non-selective reversible inhibition of cyclo-oxygenase enzymes, COX1 and COX2, and has an anti-inflammatory effect.
As the synthesis of prostaglandin is mediated by COX enzymes, studies have attempted to ascertain whether the use of NSAIDs slows orthodontic tooth movement, by inhibiting the release of prostaglandin, thereby potentially inhibiting osteoclastic activity. An experimental animal model showed that paracetamol had an inhibitory effect on prostaglandin production in the PDL, but no change in rate of tooth movement, whereas ibuprofen decreased prostaglandin production in the PDL and decreased the rate of orthodontic tooth movement.11 Whether the observed reduction in tooth movement would be clinically significant in humans is questionable.
A multi-centre non-inferiority study by Bradley et al showed that a combination of pre- and post-operative ibuprofen is better than paracetamol for controlling orthodontic pain.12 Other work has reported that the use of sugar-free chewing gum can be an effective aid for orthodontic pain management and, in fact, can reduce the use of ibuprofen with no concurrent increases in appliance breakages.13 A 2017 Cochrane review found that ‘analgesics are more effective at reducing pain following orthodontic treatment than placebo or no treatment. Low-quality evidence did not show a difference in effectiveness between systemic NSAIDs compared with paracetamol’.14
Root resorption
Orthodontic tooth movement relies on bone resorbing and root cementum remaining intact. The anti-angiogenic properties of cementum have been proposed as a mechanism by which osteoclastic resorption of cementum is inhibited, as the osteoclasts cannot gain access to the root surface area. The increased mineral content of cementum in comparison to bone probably also contributes to the relative resistance of cementum to osteoclastic activity, as well as the periodontal ligament fibres being more densely inserted into cementum than alveolar bone. Nevertheless, some element of root resorption during orthodontic treatment is likely to be almost universal, with 1–2 mm of root resorption often quoted as a normal side effect.15 Being able to predict those patients at risk of severe root resorption would be extremely useful, but as yet not possible.
Research in the early 1990s described treatment-related risk indicators for root resorption to include root torque, maxillary surgery and approximation of maxillary incisor roots against the lingual cortical plate.16
An overview of systematic reviews was published in 2021 by Yassir et al, which described the risk of orthodontic-induced inflammatory root resorption being higher for fixed appliance treatment using heavy and continuous forces, intrusive forces (especially in conjunction with anterior temporary anchorage devices), maxillary incisor torque and retraction, mechanically complex treatment of severe malocclusions, treatment of long duration and tooth-anchored expansion. There was insufficient evidence to confirm the effect of other treatment- and patient-related factors, including age and gender, unusual root morphology, history of trauma and systemic medication.17
Pulpal reactions
Changes in pulpal blood flow have been investigated in response to orthodontic forces. In a rat model, blood flow was shown to increase following orthodontic tooth movement.18 Another study using a radiospirometric method examined the respiration rate in human teeth which had been subjected to an orthodontic force for 72 hours and then a subsequent rest period of 1 week. The pulpal respiration rate remained depressed after orthodontic tooth movement, with the age of patients negatively correlated with the respiration rate and the size of the apical opening of the tooth positively correlated with the respiration rate.19 Other work has shown that following an initial decrease in blood flow after orthodontic force application, there is an increase in functional pulpal blood vessels, as a result of an increase in angiogenic growth factor.20 A 2021 systematic review found that orthodontic tooth movement does not induce loss of pulpal vitality, although with low certainty of evidence.21
Accelerating orthodontic tooth movement
Various methods for accelerating orthodontic tooth movement have been proposed, including pharmacological (e.g. hormones and vitamin D), physical (e.g. vibrational forces and photobiomodulation) and surgical. Animal studies have shown that local injection of various pharmacological agents can increase orthodontic tooth movement, but safety is a considerable issue that would need to be explored for translating these technologies to humans.
Vibrational forces have been proposed to be able to accelerate tooth movement. Vibrational forces are already used for the maintenance of bone mass in post-menopausal women or people with reduced mobility and prolonged bedrest.22 Animal models suggest that vibrational forces result in an increased rate of tooth movement, osteoclastic activity and bone remodelling within the periodontium.
A prospective randomized controlled trial investigated the effect of supplementary vibratory force on orthodontic treatment using fixed appliances and found that the vibratory force does not affect space closure, the duration of treatment, the total number of visits, or final clinical outcome.23
There has also been increased interest in surgical techniques to increase the rate of orthodontic tooth movement, based on the concept of ‘rapid acceleratory phenomonen’, a tissue reaction to a stimulus that increases the healing capacity of the affected tissues. This phenomenon was first described by Frost in 1983 and has been likened to the body's ‘SOS’ response.24 In fact, procedures such as orthognathic surgery and distraction osteogenesis probably also contribute to increased tooth movement through the same SOS mechanism. Various surgical techniques have been explored for accelerating tooth movement, including the use of full thickness flaps, with vertical incisions made between teeth and bone grafts placed, or the use of corticision or piezocision.
A systematic review found that there is low-level evidence that such surgical adjunctive procedures accelerate tooth movement and reduce treatment time, but that the acceleration is likely to be fairly minor and transient. The review also highlighted that side effects of these procedures, although likely to be fairly transient, need to be considered, as well as the costs.25
Latest developments
The mechanisms underlying orthodontic tooth movement continue to provoke interest and investigation.
A 2023 in vitro study investigated the similarities in the inflammatory processes common to both periodontal disease and orthodontic tooth movement.26 The authors found that periodontal inflammation and mechanical forces associated with orthodontic tooth movement resulted in bony breakdown by effects on different cell types, with distinct mechanisms for periodontal bone breakdown and orthodontic bone remodelling.27
Another area of recent research is developing the ability to predict those individuals who might be more prone to orthodontic-induced inflammatory root resorption by detecting possible biomarkers in either the blood or the saliva. In a small retrospective study, there was a significant increase in salivary cytokines including the interleukins IL-7, IL-10, IL-12p70 and interferon gamma (IFN-g) and a significant decrease in IL-4 for patients with moderate/severe root resorption.27 Gingival crevicular fluid has also been used in a 2021 study to identify tissue-specific markers that may allow early detection of root resorption during orthodontic tooth movement.28
Conclusion
Despite advances in our understanding of the biological processes underlying orthodontic tooth movement, there is still a great deal of detail which is unknown. The mechanisms underlying the genetic regulation and orchestration of cells, tissues and systems are still not fully understood and it remains difficult to explain why some patients respond differently to orthodontic forces in terms of rate of tooth movement and extent of root resorption compared to others. It is hoped that future research will focus on how orthodontic forces influence the genomic environment and whether individualized gene-therapy approaches to orthodontics may be possible in years to come.